In March and April this year, as the toll from COVID19 climbed, it soon became clear that we did too little too late; delayed lockdown, terrible procurement and general over-centralised dogma driven chaos as our politicians grappled with science they had little understanding of or experience with.
Now, as we are heading for Autumn, things are very different. Mortality across Europe has returned to normal levels, that is; there are no excess deaths in Europe. In Devon, there were 10 cases in the last week in a population of about 1,000,000, and no deaths.
In England (unlike Scotland and Northern Ireland) there is a general agreement that COVID19 is not going away. In other words, that eradication is not possible and that we have to get used to it – that it will become an endemic disease like flu or colds. But what does that mean on the ground?
Perhaps we have to live with a certain element of personal risk – but right now that level of risk seems very low as I will show below. So how does that square with attempts to snuff out outbreaks which are not causing serious harm in terms of hospital admissions or deaths? As we no longer need to “protect the NHS” what are we now trying to achieve?
Numbers…..
PHE are not publishing the daily deaths on their dashboard since mid July while a review takes place of what they are actually counting. (No, this is not a Monty Python sketch!) This has been prompted by potential over-counting due to people with positive tests dying of unrelated causes and still counting as a COVID19 “associated” death months later.
In some cases this may well have been relevant as recovery can be prolonged and death delayed after severe COVID19. The numbers are not huge and the main trends the same, yet potential errors are now becoming important as the numbers of deaths continue to fall and small errors play a relatively bigger part. It hardly inspires confidence.
As ever, trends can tell us more than actual numbers, and according to the ONS, total deaths over the last week (8823) are now less than the five year average (9093) with 295 deaths having “COVID19” mentioned on the death certificate.
What about its prevalence in the general population? The ONS explore community (outside hospitals or care homes) prevalence with random nasal swabs taken over the last six weeks in England and found that 116,026 swabs revealed 56 positive tests. On the basis of this, they modelled that 37,000 people in the UK had the infection in the last week, giving a prevalence of 0.07%, that is 1 in 1,500 people. Daily admissions are down to 183 people (July 22nd) with 83 in ventilator beds.
On the basis of the ONS study there might be a 3% chance of hospital admission if you get the infection, so it remains a significant illness, though highly stratified of course, according to age and risk factors.
What is happening with testing?
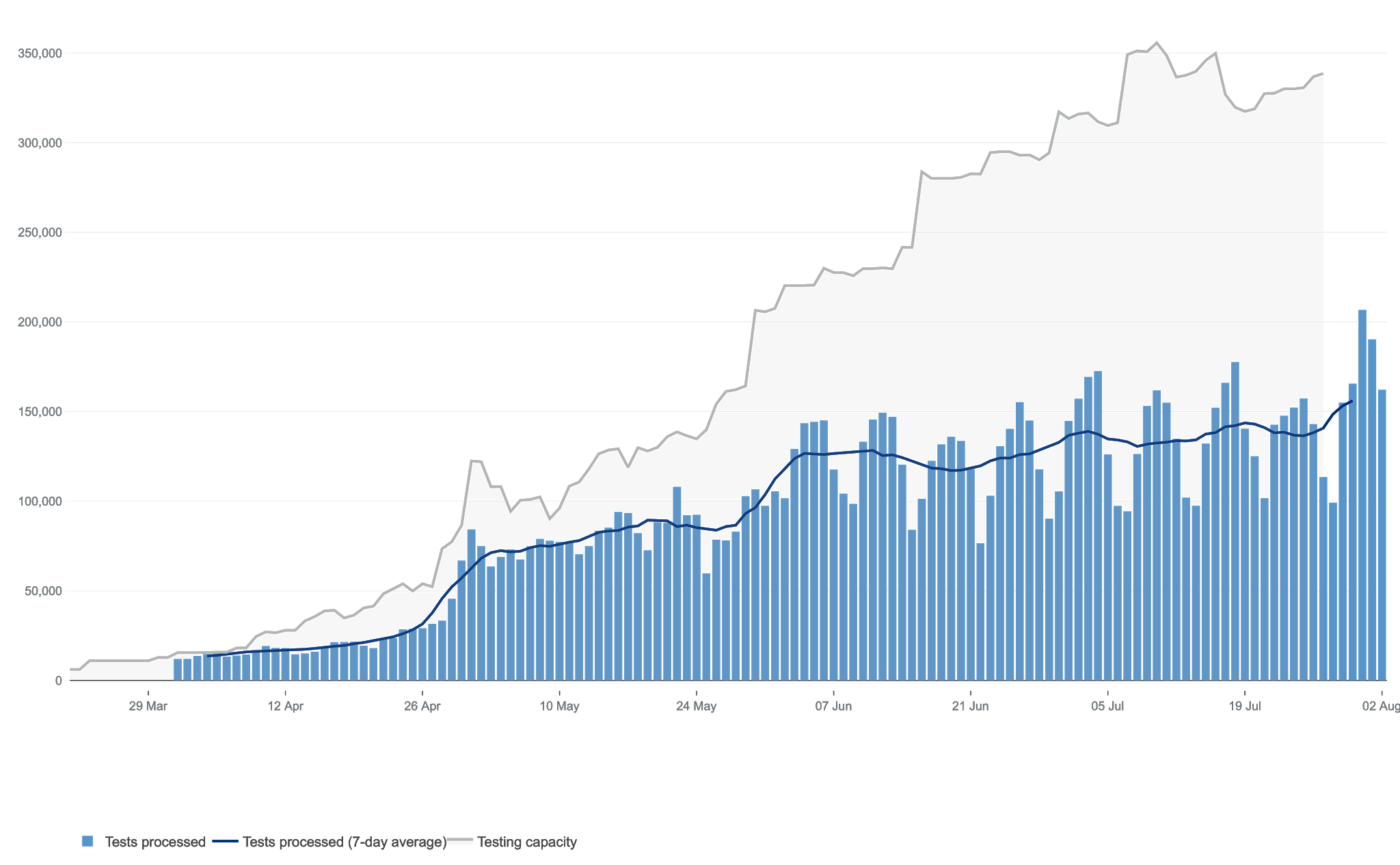
The number of tests done is increasing all the time as this graph shows:
 |
| COVID TESTS |
The more tests you do, the more positive results you will get, so is the increase in ‘cases’ an artefact of this? The graph interestingly also shows the difference between testing capacity (grey area) and tests done (blue area). That represents public funds going to the private companies contracted to do this work, much of which is for doing very little.
Testing and tracing, sadly, is in the doldrums. The Government in England have made a mess of the system. I could hardly believe the contortions of a minister trying to gloss over the cracks in the system yesterday morning. Not enough people with infections are coming forward, likely due to inability to lose pay due to isolation after a positive test, or skepticism, or ignorance. Then they are not able to list all their close contacts, and then not all the contacts are able to be traced. Each step moves away from the target needed for the system to work.
Local public health teams continue to do the majority of the graft with ‘complex’ cases being the bulk of the work, and must be very frustrated indeed. Local government, public health bodies and primary care are intentionally being kept out of the loop.
The government have effectively used the pandemic to outsource Public sector work. As Boris stated in a speech in February, there are opportunities in a pandemic for business. More on this later.
Anyway, to the results…..
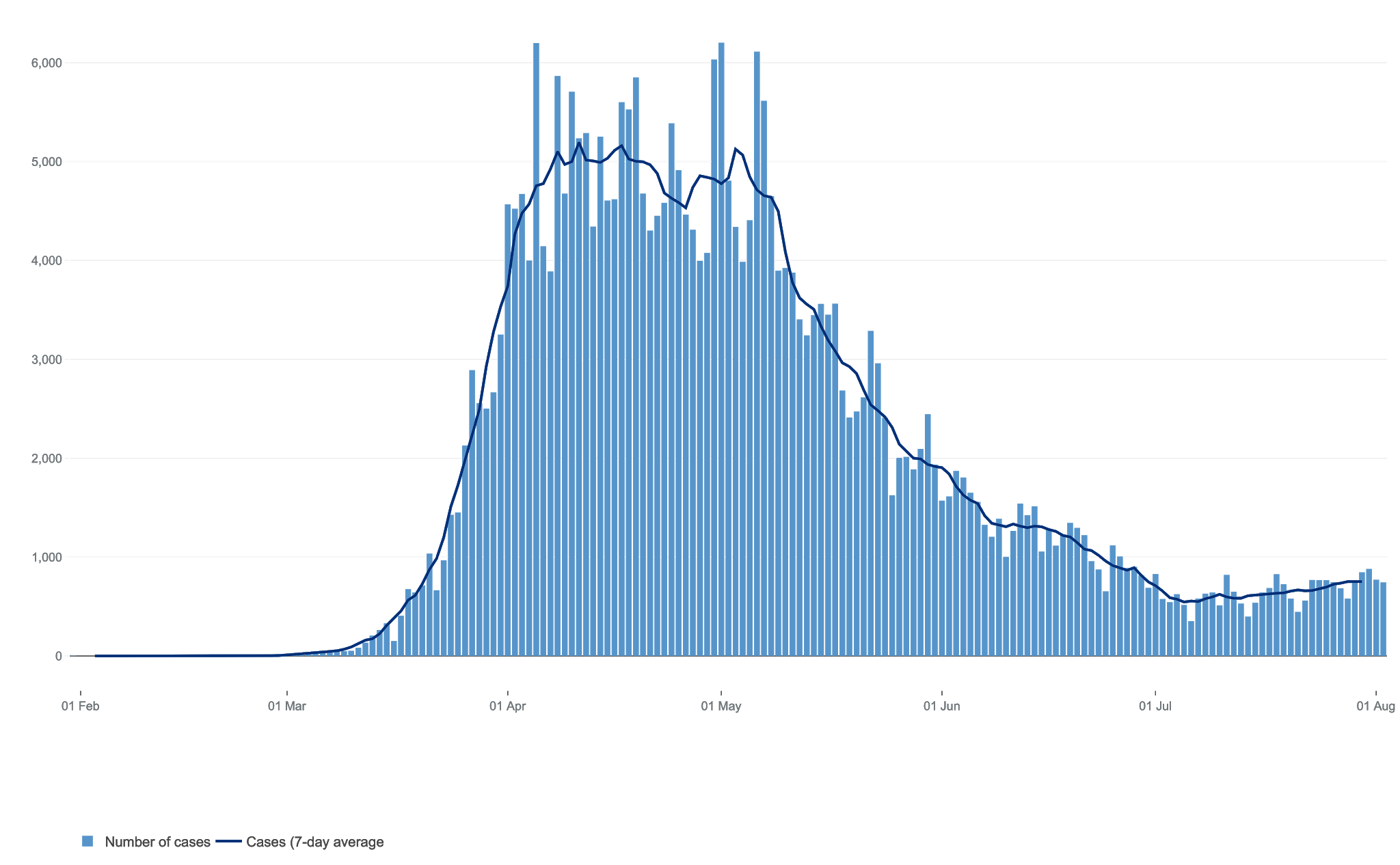
So, the total daily cases look like this
 |
| COVID 19 “CASES” |
It is to be expected that the number of positive “cases” are increasing as lockdown is released, and as the number of people tested increases. That is exactly what would be expected of an endemic infection in the summer.
Now when I was a practicing doctor, a ‘case’ meant someone with an illness, someone who came in my door with a problem. With COVID19 I’m reading everywhere about the number of ‘cases’ but this increasingly means people who are not unwell, and often being tested because of minor symptoms or if they have been in contact with cases, not, in the clinical sense, ‘cases’ at all.
We shall have to wait a few weeks to see if the increase in positive tests impacts on mortality or admissions, but I doubt it. Given its the summer, perhaps it is worth the wait before plunging into more restrictions?
What really matters are hospital admissions and deaths:
The data for these are reassuring as they continue to testify to the reduced impact of the virus in the UK.
Hospital admissions continue to fall:
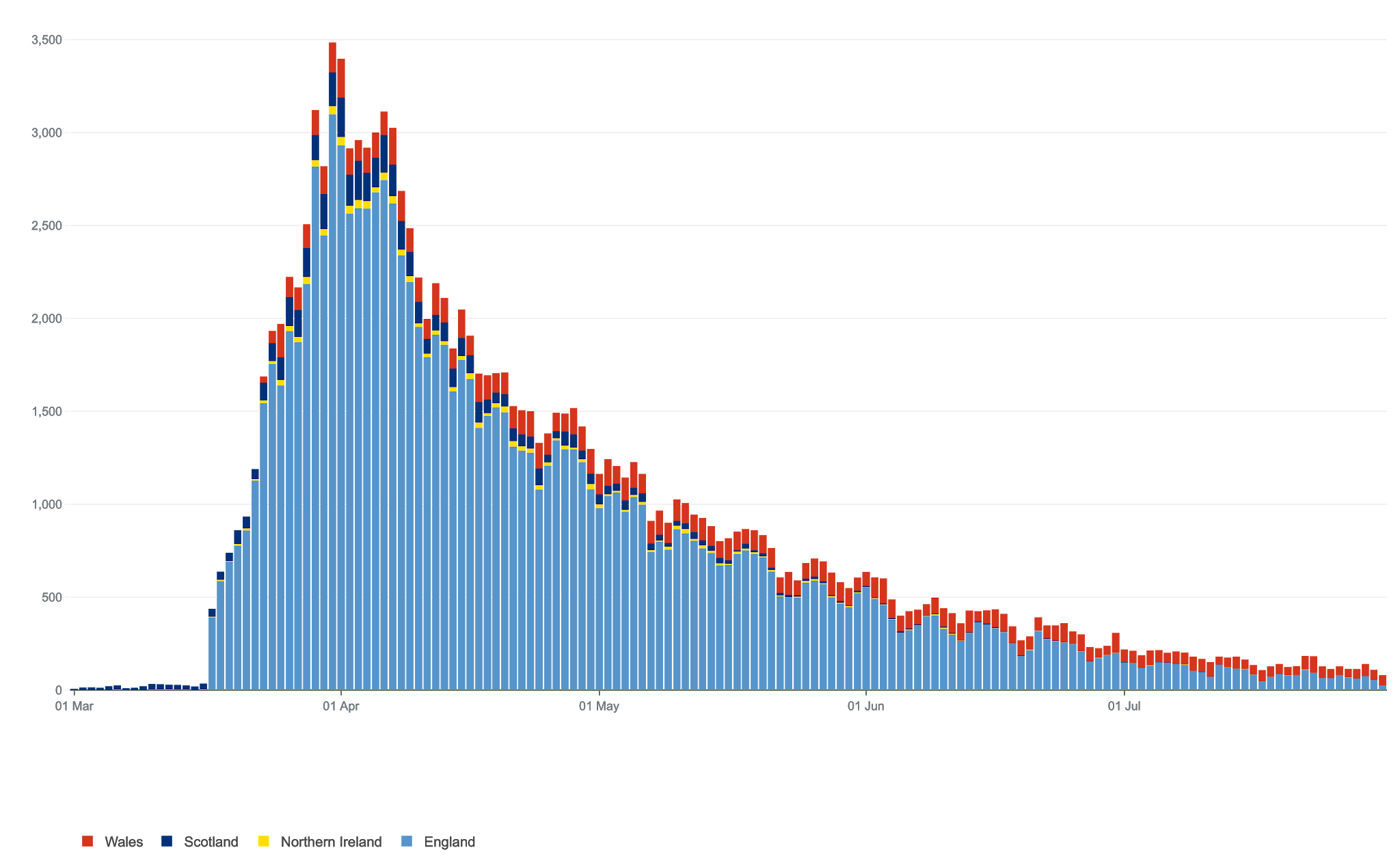 |
| HOSPITAL ADMISSIONS WITH COVID19 |
Unfortunately, we (unusually) don’t publish figures for recovered cases which would be useful to know and indeed, exclude from any further mortality figures. It would also be helpful to know how people are recovering as there are concerns that for a significant number, the illness lingers on for some time and symptoms of ongoing listlessness and fatigue can be very frustrating for those trying to rehabilitate.
Yet any discussion of a “Second Wave” is clearly off the mark right now, it there is going to be a second wave, it will arrive in the winter. Worryingly, it is only a few weeks now until children return to school and I cant help but feel the summer has been a lost opportunity to get the pandemic infrastructure of testing, tracing, isolating and supporting right.
Deaths too are now running at low levels as this graph shows
Bear in mind also that small errors in counting now make a bigger difference. Deaths with COVID mentioned on the certificate continue, but there are issues with the counting which need to be resolved soon, but the more solid data on total death, as I said above, are reassuringly normal.
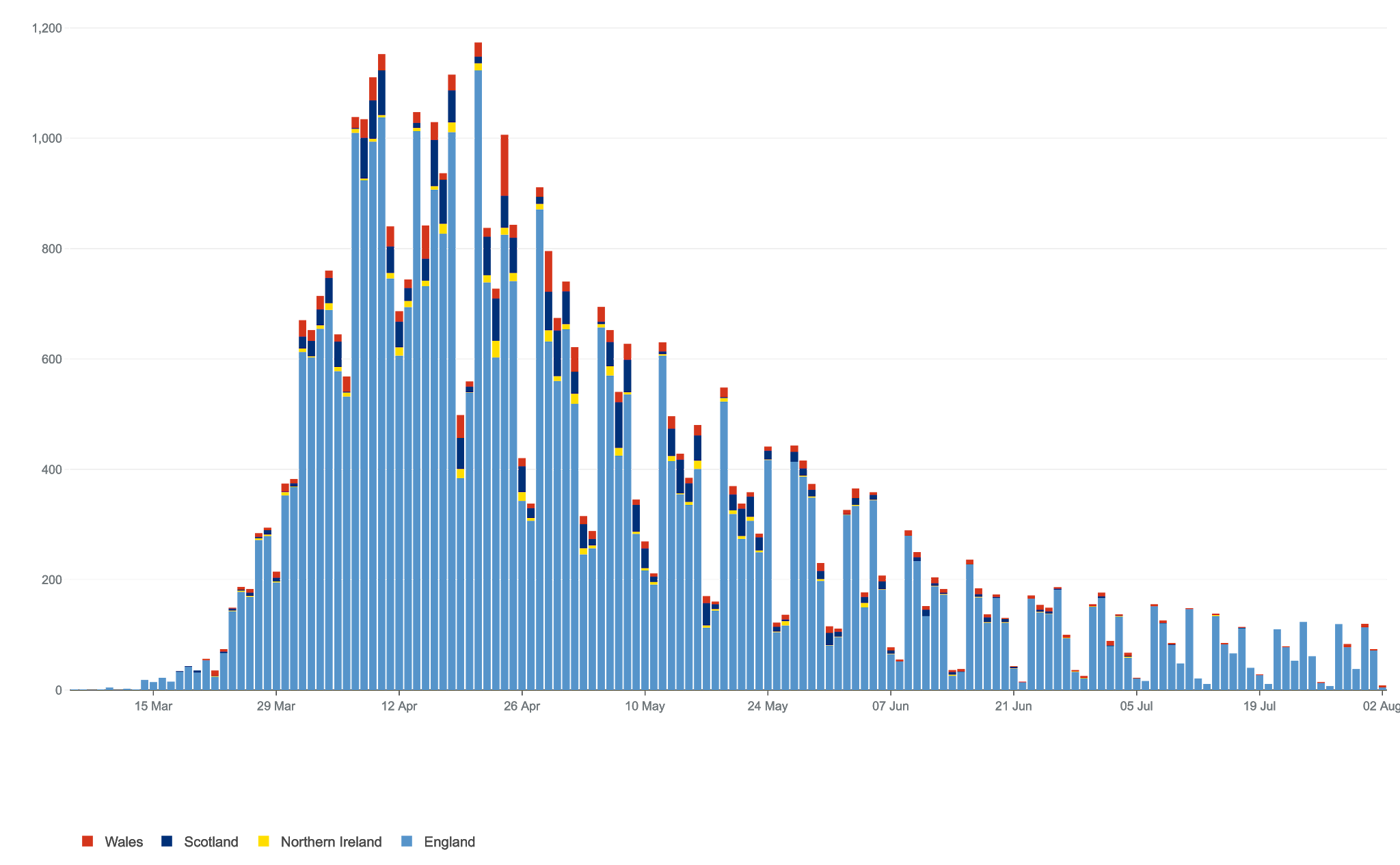 |
| COVID 19 DEATHS |
As ever, we seem to be one step behind. The initial lockdown was too-little-too-late, and now reversing relaxation of restrictions might be too-much-too-early? I wonder if they are needed at all during the summer and autumn. Winter might be another matter – I really hope it might not.
There are other encouraging factors at play…..
Vitamin D is more important than we think
Like its more benign cousins the betacoronaviruses and influenza, COVID19 dies out in the summer. For me the most compelling driver of this are higher levels of Vitamin D, and their positive effect on what is called our innate immunity – our own, inbuilt immune defences. It
{kind=link}
goes beyond common sense that this vital vitamin, so low in the winter makes a big difference, one recent paper stating:
“Population-wide vitamin D sufficiency could also prevent seasonal respiratory epidemics, decrease our dependence on pharmaceutical solutions, reduce hospitalisations, and thus greatly lower healthcare costs while significantly increasing quality of life”
This is displayed in this graphic from Dr David Grimes, a longstanding campaigner on the value of vitamin D supplementation.
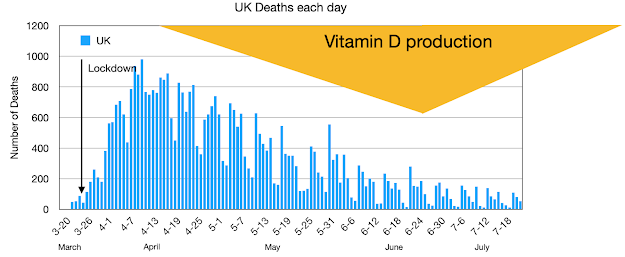 |
| Thanks to David Grimes for the image |
Lots of lobbying seems to have dragged out the recognition from the Chief Scientific Officer, Sir David Vallance, that millions more should be taking Vitamin D. I will post on this again later, before the winter, but am perplexed at the lack of interest shown by government to what has the potential to be a true game changer. Lobbying is continuing, but in the meantime, make sure you get adequate Vitamin D by getting lots of sun (most people are unable to) or supplementation with 4-5000iu Vitamin D3 daily. I will post again on this soon.
Immunity might be more widespread that we think
In another post, I wrote of the T Cells and how they target invaders like COVID19, how exposure to SARS and other coronaviruses might offer cross reactivity against COVID19, and
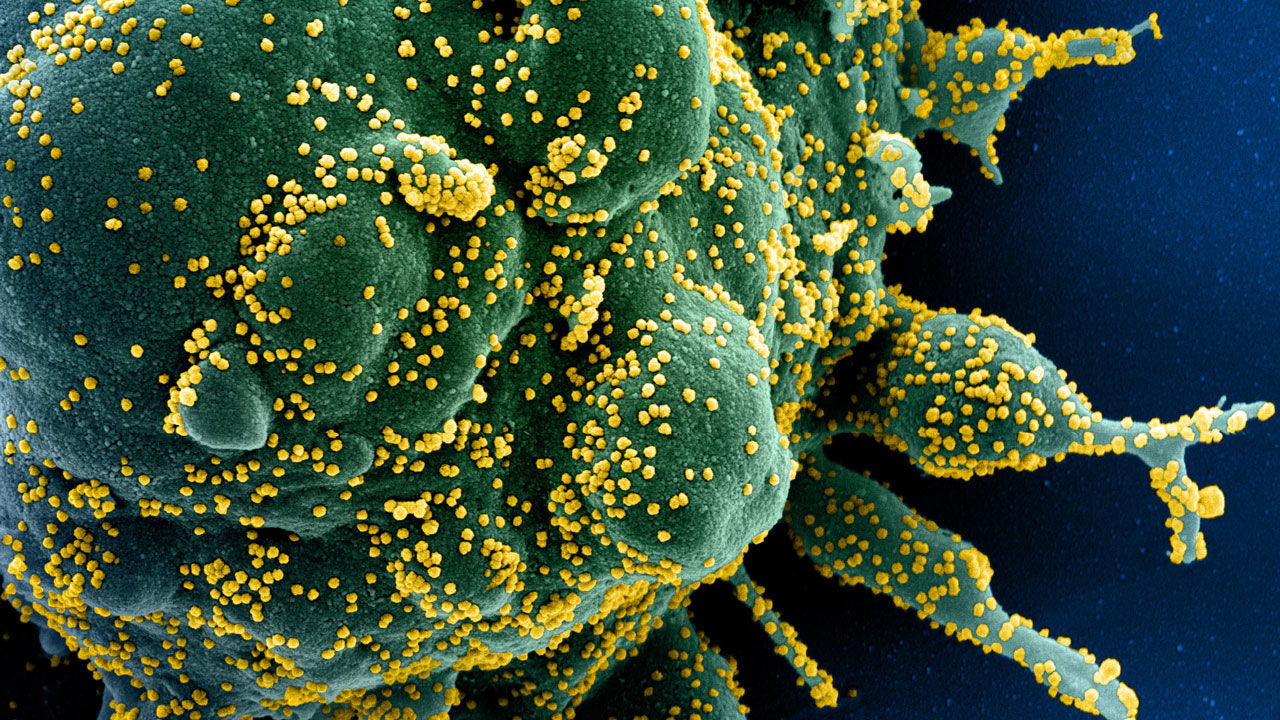 |
| T Cells (big green cell) COVID19 (small yellow objects) (Science) |
how we might be building up herd immunity way ahead of the levels of antibodies circulating in the community.
Another recent study shows that cross reactivity of T cells against COVID19 is present in the blood of 50% of pre-pandemic blood samples which might explain why some people cope so well when infected.
I hope there may be ways of testing this sort of immunity more widely, but it does also seems to explain why so many younger people are spared the worst of the illness, while us older ones tend to have run out of effective T cell immunity. (Immunosenescence)
Herd immunity might be nearer than we think
Classic ways of looking at herd immunity are changing with COVID19 and the estimate of how many people need to be infected falling according to some scientists.
The usual levels of herd immunity (80-90%) cited are for unexposed populations with no immunity to an infection, but this will be reduced by whatever protection is derived from previous infections with milder coronaviruses.


This means that is has differing impacts on different groups of people with differing exposures. The young immune do alot of ‘hoovering up’ of the virus it seems. Meanwhile, some of those those susceptible tend to get the virus early and thus are not available for re-infection. Both these effects reduce the proportion of the population needed for herd immunity. So there are suggestions that the level we need for herd immunity as measured by a positive antibody test might be as low as 20%.
“Nerd Immunity” may help
Also contact tracing through digital means may reduce spread, and thus the likelihood of coming across the virus, and therefore the level of infection needed for herd immunity. With so many of us having mobile phones we are all in this sense, ‘nerds’, and so with the right technology this might might also reduce the opportunity for the virus to spread.
There is hope this will make a difference in India and has been a significant part of the strategy in South Korean containment of the virus, as, backed up by effective epidemiological footwork it changes herd behaviour and again reduces the number of hosts for available for COVID19.
All these factors mean the virus is less likely to find a susceptible host and find itself up more and more cul-de-sacs.
Air pollution is more of a killer than we think
What about air pollution? Some of the decline, and the subsequent increase in cases be due to that wonderful decrease in air pollution we experienced in lockdown being reversed as we return to our poisonous levels of emissions from traffic and travel.
 |
| Civilisation?? |
American research suggests that relaxation of restrictions and increased air pollution takes a heavy toll on COVID19 related illness.
They conclude:
“Our results show that increased pollution nearly doubles the conditional daily COVID-19 death rate and case rate.These results are stronger for counties with higher fractions of Black individuals, lower income individuals and unemployed individuals, suggesting that the burden of pollution exposure is unequal. Pollution might have the largest impacts on the most vulnerable members of society, causing higher death rates and more severe cases of COVID-19.”
This disproportionally affects the BAME and deprived communities who have always suffered more from the significant impacts of traffic, much from the exhausts of the more financially well endowed commuters. Horribly interesting. Sadly unsurprising.
What are we doing to reduce dangerous levels of traffic – not enough. Restrictions on traffic in cities would help reduce spread, and much change is needed. Cycling is getting a much needed boost, but roads are packed again everywhere as we fail to face up to our obligations to those who are effectively, passive smoking exhaust fumes due to transport policy designed to enhance the freedom of drivers, trapped themselves in cities designed for the car.
So what is going on?
Infections are not causing problems in terms of hospital admissions and there are now no excess deaths, despite ONS estimating 37,000 infections a week in England alone.
So we have to be clear about why we are taking difficult steps to prevent its spread. The strategy is to suppress the virus to prevent a second wave, fine.
Yet as we release lockdown more cases are inevitable, fuelled, for example, by poor working conditions in meat packing plants and sweat shops and the inability of big chunks of our cash strapped population to survive on sick pay.
This will make local outbreaks inevitable unless we are ready with an effective testing and tracing system, and full sick pay for those isolating. In England we are clearly are some way from this and with current policies will not get there any time soon. With schools soon to return, ‘anytime soon’ might well be too late.
Another possibility is to aim for ZERO COVID19. Yet again, this would need much better testing and tracing, and more aggressive restrictions in regional and international travel, and is just not happening in England. In Scotland and Northern Ireland, perhaps.
As all outbreaks are local, surely we need more powerful local councils (as in most of the world) and locally rooted services to deal effectively with them. In England have sadly and intentionally all but destroyed this local infrastructure and continue to marginalise what is left of them – in favour of lucrative private sector contracts which are failing to deliver.
Coupled with that is the lack of openness about decisions. The most recent restrictions in northern England have been announced without the data which underpins them being available to local government or the public. Again, these lockdowns are sledgehammers applies to the nut of small local outbreaks which need the micromanagement that only local services can apply.
Further secrecy shrouds the development of rapid tests for viral RNA with results reported to be available in 90 minutes. Sounds good, but we have a track record of expensive cock-ups. Have the tests been scrutinised and validated? The incidence of false positive and false negative rates are essential to understand the usefulness, or otherwise of the tests quality. Errors can have big impacts on the individual and communities, but no one outside government has any idea at the time of writing as to the quality of these tests.
The only other option other than effective local management was to aim complete elimination of COVID19. In England that would require another complete lockdown until it disappears altogether, as well as isolation from other nations are who are struggling at the moment with more COVID19 infections. This is clearly not going to happen. So we need to understand that in the absence of effective eradication policies, infections will continue and inevitably increase as restrictions are removed.
So there is remains considerable uncertainly as to what awaits us this winter. I hope that immunity is more widespread than we think, that the Vitamin D message is getting across, that we are far nearer to herd immunity that we might have thought, and that a vaccine will be available for the vulnerable. If this is the case, then the winter will be manageable without destroying jobs and rendering the NHS ineffective.
It may also be possible that given some of the biology, severe restrictions now, before a real second wave comes along, will leave us weakened as the kids go back to school, as they must, and tired mentally, socially and economically.
So readers might well want to make sure they are up to date with the Vitamin D, get as much exercise and sun as possible, and get as fit as possible as the autumn approaches. Say goodbye to garbage food and say hello to better health and a higher likelihood of a mild illness if you do get infected.
While there is much to fear, there is also much to be optimistic about and it’s so important to look after ourselves, our loved ones and those around us.
Final thoughts.
We are thinking about sending a human being to Mars. We can deliver pin point bombs to any square meter of space on the planet at the touch of a few buttons. We can deliver packages to anyone ordering them within 24 hours, and do all sorts of other, incredible, totally needless and so often, destructive things.
Yet, with COVID19 we have shown new levels of collective ineptitude, particularly in the world of politics and particularly in so called leading nations boasting about “greatness”; England and the USA in particular. So many other nations are also led by some dreadful individuals.
Dealing with what by comparison in terms of effort, should have been a difficult by achievable challenge (we were warned) has shown the gulf between the emerging realities of the world and out-dated political decision making. We have had breathtaking errors and cock-ups. Dogma manufactures mistakes, incompetence and corruption.
Might a Citizens Assembly provide a better way of dealing with difficult decisions? I think so.
The real and much bigger threats of climate change and ecological destruction are increasing and the world is changing frighteningly fast; we will have to adapt more in our lifetimes that ever before in our history. Change is inevitable. Horizons are drawing in.
 |
| Bo-Jo on LBC |
I reflect on Boris Johnson briefly wearing glasses to back up Dominic Cummings schoolboy excuse for his now infamous “see if I drive my car into a wall” eyesight test and wonder if we will ever get this right.
Yet, can anyone ever be as idiotic as Trump; one day calling for less testing (and so less cases) and the next heralding the US as world leaders as they have a low ratio of deaths to positive tests (thanks to more cases). Please don’t re-elect him!!
We have the ability, but not the political will to ‘follow the science’ that is, test your best ideas, and if they don’t work, learn from them and explore new ones. We need more flexible thinking and action, better acknowledgement of the biology of this living planet and our place on it.
We desperately need better politics.
Thank you, Colin. I really appreciate this regular dose of good sense. S
Brilliant – thanks Colin!