Summary
- Sadly, we are now seeing a fourth SARS2 wave.
- Immunity from vaccination and infection will make this a lesser problem as will the summer season.
- The NHS continues to struggle and needs more nurses and cash.
- Compulsion is now on the cards for care staff and perhaps NHS staff too.
- There are grounds for optimism.
- Online scare stories debunked.
We are hearing alot about the third wave, which for me, (see graph below), is actually our fourth wave and is sadly muddying our optimistic waters. While we are uncertain as to how it will eventually look it is worth taking stock of our vulnerabilities.
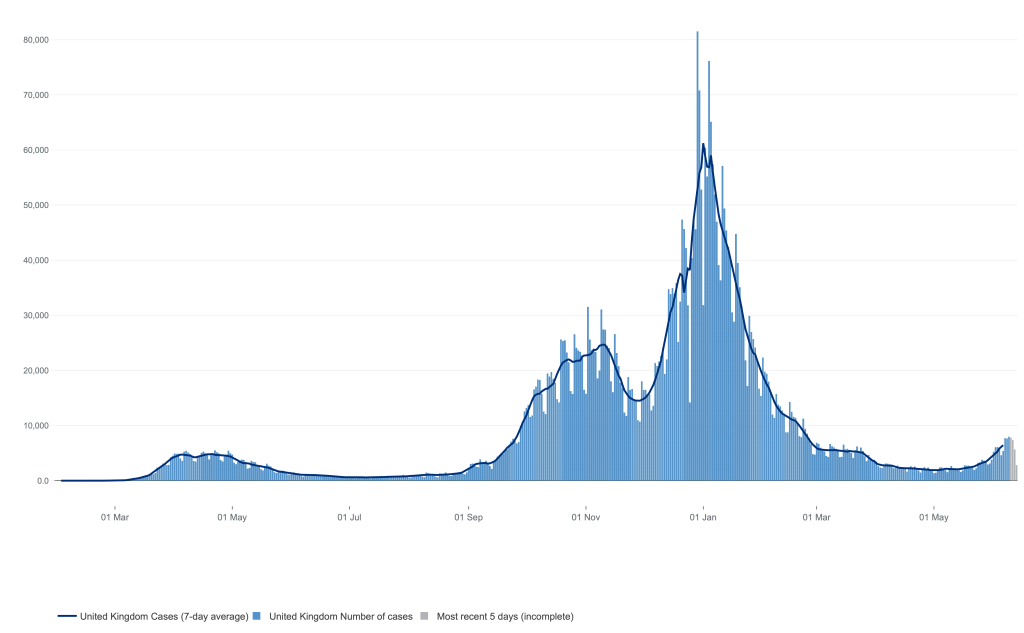
Cases are increasing enough to recognise a fourth wave, but the link between this and hospital admissions seems to have been broken and there has been no increase in deaths.
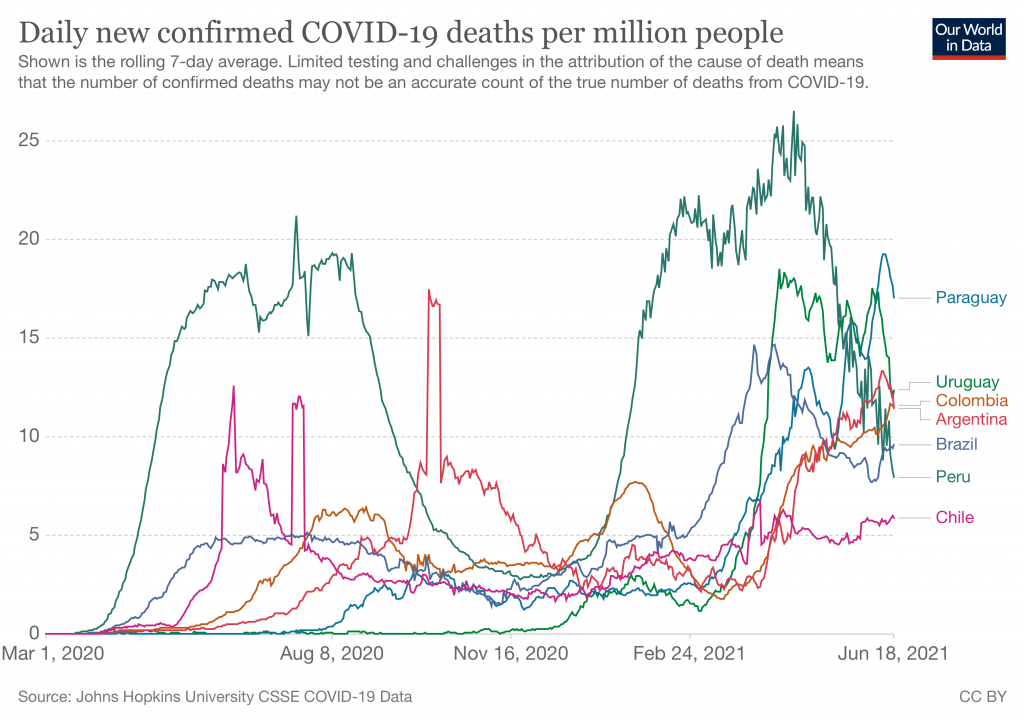
Around the world too there are problems, particularly in South America who are currently suffering badly.
Delta variant
This new variant is comprised of 13 mutations, 4 of which make it more sticky and harder for the immune system to attack. These changes in the building blocks of the spike protein make it stick to our cells receptors better and can make it easier to get into the cell by activating the spike. The spike consists of S1 and S2, the former sticks to our ACE2 receptors and the S2 unit fuses with our cell membrane. None of the mutations are new, but the combination in this one virus is what makes the variant novel. Both wonderful and worrying to see evolution in action.
According to PHE, the new and now dominant Delta variant is 60% more transmissible between household contacts, and doubles the risk of admission after infection. In terms of vaccination effectiveness, they conclude: “After a single dose there was a 17% absolute reduction in vaccine effectiveness against symptomatic disease with Delta compared to Alpha, but only a modest reduction (8%) in vaccine effectiveness after 2 doses” Hence the delay in our so called “Freedom day”.
Immunity
The React study shows that more of the new cases are in the young, with the heavily vaccinated population well protected. 78% of cases were of the Delta variant (Indian) and the rest Alpha (Kent). Once again, we are spared in the South West, with our levels of infection 5 times less than the North East. There is less MS down here too. Perhaps sunlight has a part to play in this. Maybe.
Encouragingly, levels of antibody in the community are estimated to be running at about 70% of the adult population in the UK; this will make a big difference this time, though there are big chunks of the population yet to be vaccinated. It seems that nearly two thirds of people infected with the Delta variant are unvaccinated,
Experience from the heavily vaccinated Israel is encouraging. Both vaccination and previous infection give good levels of protection against illness, hospitalisation or death three months after either. This also raised the issue of whether those with proven infections need further vaccination. They think not….
“Vaccination was highly effective with overall estimated efficacy for documented infection of 92·8%; hospitalisation 94·2%; severe illness 94·4%; and death 93·7%. Similarly, the overall estimated level of protection from prior SARS-CoV-2 infection for documented infection is 94·8% ; hospitalisation 94·1% ; and severe illness 96·4%. Our results question the need to vaccinate previously-infected individuals”
There are caveats; the Israelis used the Pfizer-BioNtech vaccine at its correct spacing of 21 days while our 12 week gap reduced effectiveness for the mRNA vaccines. We have also used the less effective AZO vaccine. They were dealing with the Alpha variant and not the Delta variant now dominant here.
So over here things might be a bit different. In a more detailed, but smaller scale study, still in preprint, an Oxford team found immunity measured by T cells, B cells and antibody levels after infection was a variable feast and waned for some of the 78 UK health care workers who they followed up over 5 months, and did so particularly in those with less symptomatic infections. The implications are that for those with asymptomatic infections, vaccination may be worthwhile, and even for those with symptoms vaccination after infection might be a good idea, perhaps in the form of a booster.
Vitamin D

Sunshine too plays its part, with Vitamin D levels increasing at this time of the year and in this glorious sunshine helping our natural immunity
Another study from Brazil demonstrated how treatment with a fast acting form of Vitamin D can reduce problems in those hospitalised, and many more people seem to be taking supplements to raise levels depressed by our indoor life and the winter. Although problems with methodology caused this paper to be pulled from the Lancet, it does add to the many reasons for taking Vitamin D, and for everyone getting safely out into the sun. That element of Sars-Cov2 which is seasonal will clearly be at a low ebb right now and will be for some months. Next winter is another matter and will define our relationship with SarsCov2, and any summer wave is a disappointment.
The NHS
There will be particular problems in some localities, such as East London, where due to hesitancy vaccination rates lag behind the rest. In those areas hospitals are bracing themselves as there are many people still vulnerable and those yet to be vaccinated. There is also our much battered NHS coping with the problems of operating with efficiency sapping COVID19 restrictions, managing patients with the illness and its complications, the usual increasing demand due to declining public health, dealing with the backlog of delayed diagnosis and treatment due to the pandemic and now a staffing crisis heightened by pandemic driven burnout. I feel for my former colleagues. The gradual sell off of GP practices to American corporations is unlikely to help the ongoing crisis of primary care which so saddens my retirement years.

Clapping and pot banging can only go so far…..
Many nursing staff have left the profession with burnout and having been insulted but pay cuts.There are 50,000 unfilled nursing vacancies in the UK and this puts yet more stress on those filling the gaps. Banging pots is just not enough. The ongoing chaos in social services continues to make life complex. With waiting lists at historic highs, the NHS can do without the 1,000 COVID cases in hospital right now, the 160 people on ventilators and the thought of building up more demand while we wait for another wave to crash is scaring ministers to caution.
Vaccine compulsion
Then there is the issue of mandatory vaccination. It looks like “Hopeless” Hancock has announced that care home staff will be expected to be vaccinated, and potentially NHS staff too. There are arguments on both sides but my feeling is that staff dealing face to face with patients have extra responsibilities towards those with vulnerabilities for who they care. Here in the UK we have good vaccine uptake without making it compulsory in a way which hardens some attitudes. However vaccines against Hepatitis B are mandatory for surgical staff and others, quite rightly so.

Not a great reason to refuse a vaccine….
Rather that diving into compulsion, some processes could be put into place to improve uptake in these key sectors. The unvaccinated should certainly be offered specific information to counter false ideas, reassurance for those worried about side effects that they will be supported and encouragement before considering sacking. Care homes are rightly concerned about potentially losing 5% of their staff at a time of recruitment problems made so much worse by Brexit.
Of course, much hesitancy stems from historical and current distrust which is entirely understandable, particularly when it comes to our much abused racial minorities who form such an important part of the care sector. That is a bigger issue.
Round up….
So for now I have gone back to looking at the COVID dashboard every day. Yesterdays 10,500 new cases and a slight increase in people needing intensive care is troubling.
With the low effectiveness of a single vaccine, the delay of a month will mean many more people will be fully vaccinated in a month as we restart mass gatherings and crowded indoor events which are so good at facilitating spread. Yet with 70% people are at low risk of experiencing a problematical infection, and many of those in high risk groups are now covered. It seems the simple question of allow those people to get back to a normal life has some very complex answers.

Social distancing, Tartan army style
The Tartan Army seem not to be too concerned about social distancing, which is fine, but indoor events and large festivals are more of an issue as insurance is needed to help with the viability of a sector which has born the brunt of restrictions.
Would it involve some sort of certificate of infection or vaccination? Perhaps the little card I got on completing the second jab would do for almost everything, though this could, no doubt be easily copied and might need other ID to prevent those vaccinated lending theirs out to chums and the many other potential fiddles.
Perhaps this will be how things will be. More waves as variants spread from the 88% of the world people who are not yet vaccinated, until more widespread levels of immunity build up. Unless that is, we have genuinely vaccine and immunity escaping variants, and even then there is hope there will be enough immunity to make it a different experience from before. So there is much hope that that things can get back to normal. Yet for me that is when post covid life becomes more complex and more worrying again with climate change being a herd of elephants heading towards us as we shelter under our coffee tables.
The Banana world
Just an end note to mention some things not to be concerned about.
With our crazy world provoking unprecedented levels of anxiety should we add the “thousands of deaths” some are attributing to the vaccine. Absolutely not! There are dangers and deaths associated with vaccines, but these pale into insignificance compared to the real infection. Nothing comes for free, but I gasp at the ethics of some pundits trying to scare the living daylights out of the population.
Another issues is the claim that the spike protein in the vaccine is a direct cause of significant illness? Again, definitely not! Fact checkers are really useful and some really impressive ones have sprung up by many who se the antivaxx movement as essentially spreading lies. Channel 4’s recent documentary does a good job in exposing charlatans, with the truly dreadful Wakefield shown as the worst sort of doctor there is. Playing on peoples problems and experiences for his own aggrandisement and enrichment.
The online world is full of incredible garbage and Im exasperated and fascinated by “world leading doctors” announcing their theories to the world. That they have them immediately shot down by good science does not undo the mind damage which can be created by some of these sensational concepts. It narks me that the advocates of such stuff simultaneously criticise “The Fear agenda” while intentionally creating their own.
