Summary
- Researchers in Barcelona trialled the effect of Vitamin D treatment on the risk of admission to ITU and of death in patients admitted with COVID9 during the first wave last May.
- They found that treatment with Vitamin D reduced the risk of admission to ITU by 80% and reduced overall mortality by 60%.
- The results have make headlines but there are flaws in the study – the Lancet have withdrawn it from their pre-print platform pending further analysis.
- Vitamin D given to COVID19 patients in Brazil failed to have an impact, but the treatment was given too late in the illness.
- Levels of vitamin D correlate to disease severity and outcome so it is sensible to supplement with Vitamin D before you get to hospital.
Introduction
It’s so good to be on the downslope of what could potentially be the last wave of this winter. With vaccination racing ahead, at least in the rich nations, there is evidence that this too is reducing the risk of death in the most vulnerable groups. To add to this good news, a study has just been pre-printed of the results of treatment with Vitamin D and the outcomes after hospitalisation with COVID19.

Following a smaller and encouraging trial in Cordoba, researchers in Barcelona scaled up the trial to look at the effect of giving patients admitted to hospital a fast acting form of Vitamin D.
The results seemed really good news on first reading, but it seems the trial has raised interesting criticisms about how it was conducted. There is a real possibility it may not get through the peer-review process due to some significant and frustrating design faults.
What did they do?
The study included 930 patients admitted to hospital with COVID19 last April – May. Those in the treatment arm were given Calcifediol on day one with subsequent booster doses, all other treatment was the same in both groups.
They had 8 COVID wards in the hospital and in 5 of them patients were given vitamin D and in three, they were not. This is called a cluster controlled trial.
Interestingly, they measured Vitamin D levels on admission and found that 66% had levels less than 50nmol/l, potentially indicating deficiency, although it is known that infections and inflammatory disorders can lower Vitamin D levels.
What did they find?
Overall, admission to ICU was needed for 110 (11.8%) of the participants and 10% of the patients died.
Of the 551 treated with Vitamin D, 30 needed admission to ICU (5.4%) as opposed to 80 of the 379 controls (21.1%).
They also found that the higher the blood level of Vitamin D on admission, the lesser the risk of admission to ITU – a higher level about halving the risk.
Mortality was 3.6% in the treated group, 15% in the control group. After adjustment for age the reduction in mortality was 60%.
There were no significant adverse effects and the cost of treatment was very little.
Their conclusions;
They conclude: “In this open randomized study conducted during the first European outbreak of the deadly COVID-19 pandemic, we have observed that, in hospitalized COVID-19 patients, treatment with calcifediol reduced the requirement for critical care by more than 80%.
This supports the conclusion of a prior pilot trial in Cordoba in which calcifediol treatment lead to a reduction of more than 50% of ICU admission in hospitalized COVID-19 patients13.
Furthermore, calcifediol started at the time of hospitalization (intention-to-treat analysis) reduced mortality by more than 50%. Importantly, our results indicate that early calcifediol administration, prior to ARDS development, is critical for mortality reduction, since initiation of calcifediol during ICU admission did not modify patient survival.”
My conclusion
I must admit to be feeling the same sort of frustration I felt after my diagnosis of MS when I searched for the evidence of a definitive trial of Vitamin D and MS to find that few really high quality trials have been completed. Far too many studies were small scale and poorly done. Perhaps Vitamin D it is just too cheap and readily available for anyone to invest in the significant resources needed for a high quality, long term trial.

Nevertheless, there is lots of biological sense in taking it and plenty of indirect evidence too. So I have been taking 5000iu daily for 7 years now and all well so far. A trial of vitamin D in COVID19 should be really straightforward.
So it seems, despite the headlines there are some problems with this study. The really troubling thing that jumps out at me is that it was done last May. Given the sensational results, why has it taken so long to get it even to the pre-print stage?
If the results were really that good, how many lives could have been saved throughout the world if the results had been shared early last summer? Would word have got around in the local area about how good the treatment was? Was treatment continued in the hospital where the trial took place?
Why also were the patients randomised according to which ward they were admitted to? Why 5 treatment wards and 3 non treatment instead of an even 4/4 split? Perhaps the wards had different admission policies, or other differences. Why not have genuinely randomised patients alternately as they were admitted, and why not give a placebo? These aspects of the study are disappointing and I do wonder if the article will get past the peer review process.
I remain impressed by the results, and the significance of Vitamin D lack which is so common in early spring, even in Spain. It is a shame to have done such a big study without crossing the t’s and dotting the i’s and making it more convincing to medical science.
Nonetheless, the results do seem to back up the earlier smaller study, and it seems a larger randomised trial still recruiting in Spain, though with cases falling this will need to go international. Fingers crossed we are past the worst now and its findings will be relevant to the next wave, or the next pandemic?
Other recent evidence?
There is more encouragement from a recent study of 8,200 COVID cases in the UK Biobank study which found a 34% reduction in the risk of COVID19 illness in those taking Vitamin D3 supplements.
They conclude:“In this prospective study, we observed that habitual use of vitamin D supplements was associated with a lower risk of COVID-19 infection, independent of lifestyle, socio-economic status, prevalent chronic diseases, and circulating vitamin D levels”
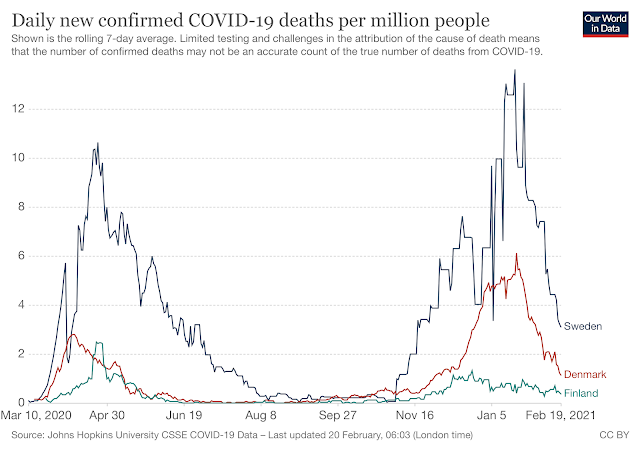
Interestingly, Finland are the only nation to significantly fortify foods with Vitamin D by law, and their mortality rates from COVID19 are very low, even compared to their neighbours. This, of course it not proof, just more encouraging evidence.
In a well conducted study in Brazil treatment with intravenous Vitamin D3 had no effect on length of stay, admission rated to ITU or death of patients with COVID. The study included 240 patients who were moderately to severely ill with COVID19 during the Brazilian winter.
The big problem there
was that the dose was given on average, a whopping 10 days after onset of symptoms and it is clear from the results in Barcelona that treatment makes less if any difference later in the illness. Perhaps patients in Brazil are admitted later in their illness? It is not clear if the patients were randomised on admission. They are randomised in blocks of 20, so perhaps there were delays?
If, 10 days after symptom onset things are getting worse, it can be assumed that patients were entering the ‘cytokine storm’ phase of the illness which is rather too late to treat with Vitamin D. The authors agree that their study doesn’t mean that earlier treatment with Vitamin D might not help.
The CORONAVIT trial has been running in London since October and will publish results in March. This looks at the potential of VitaminD to reduce the risk of COVID19.
They say: “..the CORONAVIT trial has the potential to give a definitive answer to the question of whether vitamin D offers protection against COVID-19. Vitamin D supplements are low in cost, low in risk and widely accessible; if proven effective, they could significantly aid in our global fight against the virus.”
So what to do?
For me, it continues to be really important to supplement with Vitamin D so that levels are normal before getting ill. The results from the Barcelona study are encouraging, even if the methodology is disappointing.

It also makes sense to spend as much time outdoors as possible and get as much sun as you can without burning. Thats not much of an issue right now in the wet cold north. Yet even in the summer most people live an indoor life due to work patterns and weather. This means that Vitamin D levels are lower in western populations that in people who spend more time outdoors.
In terms of anthropology, we are designed to be outdoors all day and in most weathers. Light skin evolved to maximise our intake of the sunshine vitamin with as well as bone health, brings benefits for mood, wellbeing and sleep.
Dark skin in our British climate effectively blocks Vitamin D synthesis in the skin. I fail to see how the widespread Vitamin D deficiency seen in the BAME population could not be a part of the impact of COVID in those groups. As described in my previous posts on Vitamin D, (type Vitamin D into the search box to see) supplements continue to make sense.
So there is a reasonable biological basis for the benefits of Vitamin D and great potential in minimising the impact of infection with Sars-Cov2, but the Barcelona study rather leaves me feeling that they missed a chance to gain wider acceptance of Vitamin D treatment. The Brazil study hints not to leave treatment till it’s too late.
So as I look out at todays wind and rain, I will continue with my 5000iu of D3 daily. This is now pretty standard advice for people with MS. As soon as the rain eases off I will be outside and enjoy any thin winter sun I can find. As the year moves on I will take every opportunity I can to be outdoors as we enter, hopefully, the sunny post COVID spring.