Summary
- Sars-Cov2 is evolving more rapidly than initially hoped.
- The new mutations are likely to have changed the course of the pandemic.
- It is a horribly interesting example of evolution before our eyes.
- Indiscriminate use of antibody treatment might be implicated in this.
- Vaccine manufacturers will have to keep up
Introduction
Well, as far as the pandemic is concerned it is not been a very Happy New Year.
The ominously names NERVTAG (New and Emerging Viral Threat Advisory Group) warned early in December that a new SarsCov2 variant called B117 has been circulating since September and is thought, pending definitive lab tests, to be more transmissible. Some virologists argue that in purely scientific terms it is too early to say if the new strain will mean more illness, or more severe illness. So far the signs are not good as shown by the number of patients in hospital with COVID19:
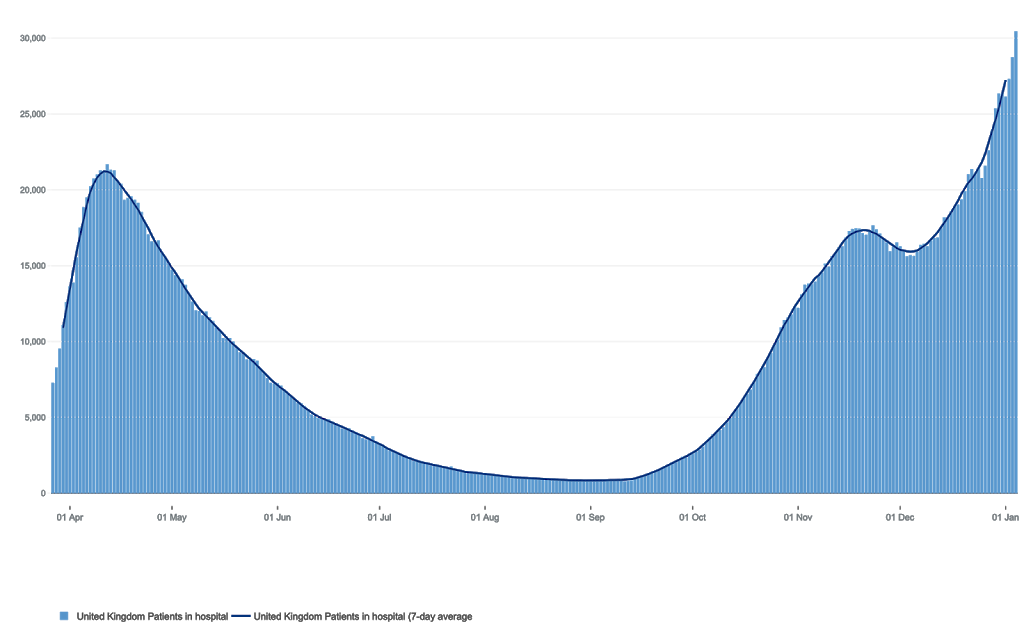 |
| COVID 19 patients in hospital – Jan 6th 2021 |
Whether due to the new strain, increased human contact, dry cold weather, or Christmas, increasing cases, pressures on hospital and ITUs now spilling over from one region to another, means a sad hello to Lockdown 3.
The mutations
There are two main variants causing concern right now are here without home grown B117, and in South Africa whose 501Y.V2 variant has already spread to 5 countries. They include multiple changes in the genetic code, with some omissions and changes in the resultant proteins whose instructions for assembly those genes carry. Improvements (as far as they are concerned) results in being able lock onto ACE2 receptors better and possible evade out immune systems.
 |
| New Sars-Cov2 variants |
As far at the UK variant is concerned, it seems there are now three large ‘clades’, (that is families or branches), with a total number of 1623 genomes (genetic instruction manuals) within them. This diversity is common among viruses – but why have so many come about so suddenly?
Initially it was hoped, indeed observed that Sars-Cov2 was more stable than many RNA viruses. This has the advantage of being able to make vaccines targeted at well defined parts of its structure. It had the disadvantage of meaning that it would not evolve into a less dangerous form any time soon. The natural history is to become more transmissible and less dangerous, but this is not guaranteed. So what’s going on….
Real time evolution..
First, evolution – random mutation followed by natural selection with whatever mutation most suited to the surroundings replicating the most efficiently and becoming the most numerous.
Secondly, what evolutionary event has led to such a significant set of mutations at once? One plausible hypothesis is that in an immunocompromised person the virus hung around for some time and was treated with convalescent sera. While this does not seem to work in terms of trial results, they have nevertheless been used – for instance, in Donald Trump. His treatment seems a recipe for creating new viral variants.
 |
| Convalescent sera – not such a clever idea? |
What happens is that all the viral strains that are sensitive to the antibodies are wiped out – in a short sharp infection, that is usually the end of the line for that patients population of viral visitors. However, when they have been busily replicating in the same host for weeks, mutations will have had more time to occur, so the viral population in that individual will have become more diverse.
The antibodies created by the immune systems of people infected with the strain previously dominant (convalescent sera) might not work against one or more of the new mutations and hey presto – a new variant is born.
Antibiotic resistance all over again
In summary, it is a classical biological tale much akin to antibiotic resistance – only happening more quickly:
1, The immune defences of certain individuals are not strong enough to kill their viral population
2. Prolonged infection leads to a more diverse viral infection.
3. Highly specific antibodies given at high concentration eliminate all the viruses which are sensitive to it.
4. A new, antibody resistant population of viruses is born.
This worrying phenomena of rapid evolution is well described in a recent paper, the authors of which conclude:
“These data reveal strong selection on SARS-CoV-2 during convalescent plasma therapy associated with emergence of viral variants with reduced susceptibility to neutralising antibodies”
What it means
Well, if the increased transmission is due to the new strain, then it’s a giant step backwards. Even though it might not lead to more severe disease in an individual (fingers crossed for that), it leads to a more severe pandemic with more cases, more illness and hospital services pushed beyond their ability to provide facilities for the many other illnesses needing immediate and urgent care. Hence the Lockdown 3 – the latest example of being one or more steps being the virus.
It must also mean that treatment with convalescent sera should, in my opinion, be abandoned or only used in the context of clinical trials to establish its place.
The other big implication is that with the virus seemingly mutating more frequently than initially thought, vaccine effectiveness will have to be continually monitored. Reassuringly, vaccines generate lots of different antibodies to the spike protein, so its a tall order for the virus to evade them all,
If any changes are needed in the mRNA of the Pfizer or Moderna vaccines, or the genes carries by the viruses in the Oxford or Sputnik vaccines to keep up with the evolution of Sars-Cov2, it will might lead to the need for repeat vaccinations. More on that later.
I keep my fingers crossed for a mutation that will lead to less severe illness, even at the cost of more rapid spread. This occurrence, of course, is not encouraged by lockdown measures, which prevent spread, but don’t allow the milder strains to do what evolution would have them do – become dominant. The spaces available for new cases in modern well equipped ITU’s are driving this policy, it seems they are the last resort of political decision making.
The scenario of low community prevalence backed up and created by Finding, Testing, Tracing, Support and Isolation to actually keep control of the pandemic seems, right now, to be an almost Utopian concept for us in the UK. For that, I’ve given up crossing my fingers.
