and on the other hand……
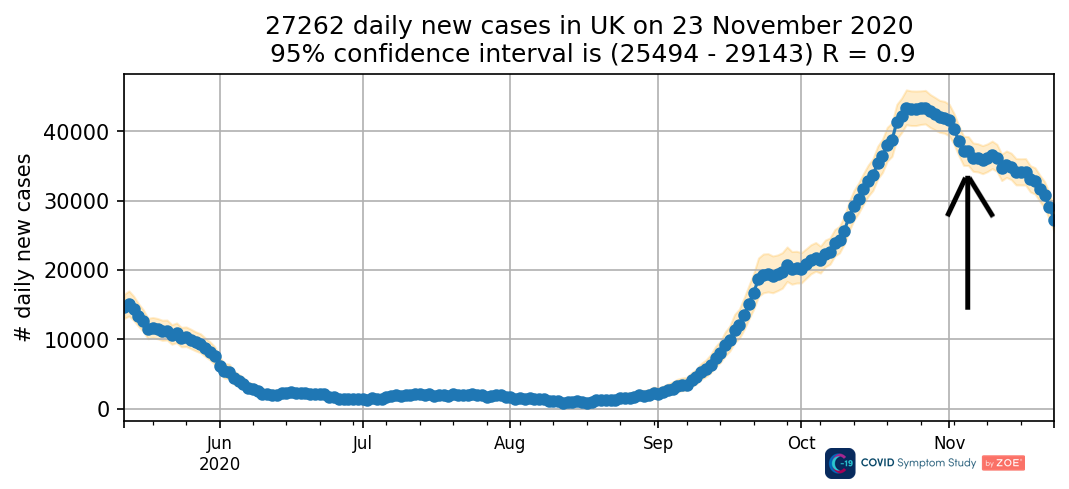
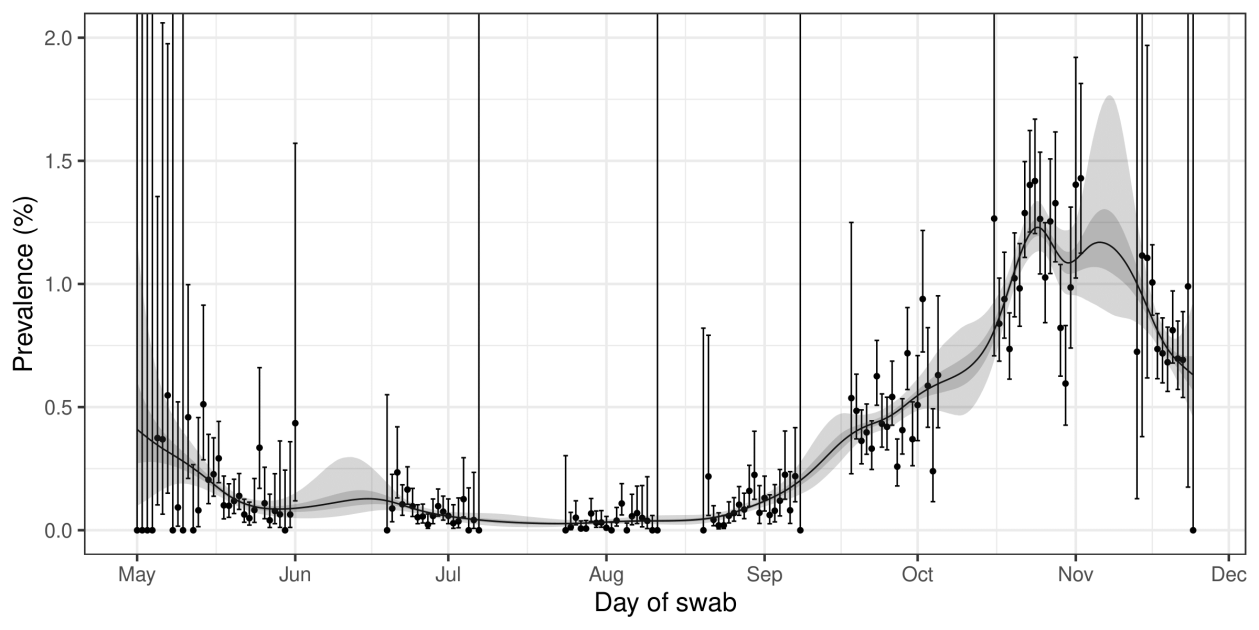
Imperial is also conducting a random sample of positive PCR tests in 100,000 people in the community called REACT-1. This survery of swabs in the community reveals a similiar pattern of positivity over the time of the lockdown though with a very different conclusion:
They show that the lockdown has had a dramatic effect on the prevalence of COVID19.
“Three weeks into the second national lockdown in England there has been a ~30% proportionate reduction in prevalence overall, with greater reductions in the North. As a result, inter-regional heterogeneity (differences) has reduced, although average absolute prevalence remains high at ~1%. Continued monitoring of the epidemic in the community remains essential until prevalence is reliably suppressed to much lower levels, for example, through widespread vaccination”
Interestingly, they do acknowledge that restrictions forcing people to stay at home adversely affects those in crowded houses where being shut indoors will lead to more cases. Measures to combat this, namely offering alternative accommodation for people who can’t effectively isolate at home have not been put into place.
Does Lockdown work?
Of course it does, but I can see the arguments from both sides. The most compelling evidence for the positive effects of lockdown include an increase in cases and infections in North America after Thanksgiving as well as the ongoing carnage in lockdown light USA. In reality, they are still in their first wave and experiencing record levels of infection and deaths from COVID19 with many hospitals struggling to cope.
 |
| Lockdown light USA COVID deaths |
While there is more to this than restrictions: poor public health, world leading social inequality, terrible food and obesity, the sad upward march of COVID related deaths is truly Trumpian.
But there are other factors too…..
Why is this happening?
Behaviour. As Tim Spector says, personal behaviour makes a difference. Whatever we think of the tiers, we have pretty much all changed our behaviour in ways unthinkable a year ago. When local hospitals are filling up, many of us who can will make big changes in the way we behave and this will particularly apply to those who are vulnerable.
National restrictions add to this. Social distancing, the wearing of masks and hand washing make a difference to viral spread and have become the norm.
Immunity. Coupled with our changed behaviour, there is clearly immunity out there. This can be seen in the very low rates of recurrent infection and the lower rates in areas hit by the first wave. While levels of antibodies remain low, and fade with time, T Cell immunity is likely to be more common and longer lasting. The reason for the relatively low mortality rate compared to other epidemics, is the existence of pre-existing immunity to coronaviruses.
Vitamin D. I would love to think that vast numbers of people are supplementing with Vitamin D. Im sure some some are and this too will make a difference. Hard evidence of community uptake is difficult to come by and advice from our leaders is way behind the science. Lots of evidence is accumulating regarding the effectiveness of Vitamin D, and we are missing the opportunity to correct this most modern of health problems in time for COVID19.
Natural pandemic history. The other thing of course, is the natural history of pandemics. We will only know this for COVID19 in a year or so when we look back at the now fluid graphs as they are frozen by time.
So, what of the natural history of past global viral pandemics? The biggest one in the last century, was the 1918-20 H1N1 influenza A pandemic. This hit the world in three waves, the second bigger than the first, and was fuelled by movements of young men from all areas of the world to concentrated super-spreading military training camps. It it hypothesised that more deadly strains were selected out by the extraordinary circumstances of the war turning normal behaviour upside down in epidemiological terms.
Instead of the ill staying, and dying at home, those soldiers with mild cases were kept in action, relatively isolated at the front, while those who were ill were taken to field hospitals and then back home, spreading the disease during every phase of their journey.
With little immunity from previous flu outbreaks, the 20-40 age group were particularly affected with truly terrible consequences for a world struggling to recover from war.
The natural history of this illness can be seen from the graph below, from a review published in 2006.
 |
| 1918 Influenza pandemic waves |
Of course, that pandemic was different, yet immunity built up and the pandemic ran its course, tragically leaving 50 million dead behind it. By comparison, COVID19 is a milder infection, though at least 10 times worse than endemic flu strains, most of which have descended from the 1918 pandemic strain. COVID19 will come in waves, perhaps up to four, then fizzle out to join flu as a part of our year to year experience. To some degree this has to be what we are seeing right now. Hope that its severity will decline with time is right now, hope, not certainty.
Further, those who say we should maximise ‘freedom’ at the expense of the ‘vulnerable’ seem to fail to understand the dangers of overloading of a fragile, poorly prepared and understaffed NHS which can provide care for so many people and in so many ways not imaginable in those sad days after World War 1.
However, with the costs mounting surely we could better balance the needs of the future with the present and allow more human and social activity. Perhaps based on more finely tuned, locally applied measures, and like in Scotland, a wider choice of tiers, and dare I say it again, a functioning way of providing specific advice to individuals with infection with testing and tracing.
How could we do better?
Taking Away Control – Localism. One complaint is that the county wide application of Tiers is too broad a brush. Our over-centralised approach is again reflected in restrictions applied to large areas containing very variable rates of infection. Power and control have been taken away from local councils and this politically driven phenomena is playing out with the pandemic.
Yet, local Authorities are better placed not only to decide on restrictions needed to keep hospitals functioning, but also to change levels on the basis of local outbreaks and hospital capacity. That Boris feels that this would simply be too complicated for people to understand is a testament to the cobweb laden weakness of centralised diktat. Patronising is too weak a word for it.
Both lockdowns offered the opportunity to enhance testing and tracing and once again this has been sadly missed. Our testing and tracing system has morphed into a resource devouring incompetent monster. Mass testing comes to mind.
Mass Testing?? The outcome from that chunk of the £500 million spent on the Innova lateral flow tests used in the Liverpool experiment is that a few asymptomatic cases have been found who were less likely to be spreading the virus in any case.
Does it work? I and many others don’t think so. The British leading the world? Innova is a odd creation: It is registered in liability-light Las Vegas, set up by an obscure investment unit in Hong Kong and makes the tests in China. As stated in the Private Eye, it is very good at lining pockets.
The test is not without its flaws. There are few false positives (0.3%) but far more false negatives. The test missed 20% of people infected with the virus when performed by skilled staff, and surprisingly for a “simple” test, this increased to 40% for those self testing. So about half the COVID cases will slip through the big holes in this net.
 |
Testing (and spreading?) event in Liverpool
|
Even the small false positive rate matters when the test is applied to large numbers of people, only a few of whom will be infected. For example, if 100,000 people are tested in an area with prevalence of infection of 400/100,000, the test will give 630 positive results, though only 230 of them will have COVID19.
Like the other data above, the cases were already in decline before the army arrived to administer the tests. Recent analysis shows the trial has failed, and should be stopped. Despite the financial resources and effort expended on weekly mass testing, Liverpool is still facing Tier 2 restrictions, so the benefits are hard to see.
Despite the lack of benefit there are plans to roll it out across the country, and this could cost a staggering £100 billion. This equates to £3,500 for every household in the country. You don’t have to be an economist to gasp at the sums being delivered to the private sector without much evidence of an impact. Imagine how much more value these vast resources would have returned if invested in other sectors, for instance, restorative farming to repair the countryside or carbon capture to lead the world in sinking carbon.
Perhaps the technology would be better targeted at healthcare workers and possible students, but should really be subject to evaluation first – this must be particularly galling for the National Screening Committee, a body already set up and tasked to do this job, yet rather like primary care and local public health, not even asked.
More tiers. Following Scotland’s lead in having more Tiers to apply would also have helped. I suspect that would have been seen in Downing Street as following the SNP’s lead and thus politically unthinkable for this government. With the NHS app and technology the way it is, more flexibility of a larger number of tiers would have meant less restrictions in many areas.
So do the costs outweigh benefits?
I admit that it’s no easy matter for politicians to plot a way out of this. Rishi Sunak’s sunny days seem over now. Its one thing splashing the cash, inevitably popular, but another to work out how to pay it back. His recent financial statement hints at pain to come and delivers that pain now for key public sector workers already demoralised by a decade of frozen pay and worsening conditions.
 |
Jam today,
Toast tomorrow? |
Those costs include the haphazard and declining quality of the education of our children. Teacher attrition is likely to increase from its already unacceptable levels. Every year 20% of teachers leave the profession. This matters. Prevention children playing in the park matters and adults socialising too. Businesses and livelihoods will be sacrificed.
Another month, or months of restrictions will need to be accompanied by a financial package of support for small and medium enterprises which have long been recognised as central to our economy. One demonstration of how this has impacted them is how they have missed out on the recent rise in retail sales, most of which has gone on-line to Amazon, whose effects in economic terms is that of a giant wealth extracting parasite. Sadly, their profits have tripled during the pandemic.
If we are going to continue with what is called orthodox Conservatism the economic pain will outweigh the gain, many many times over. Perhaps the time has come for new thinking – a Universal Basic Income, for emergency “Quantitative Easing” to clear COVID19 related Government debts. Perhaps, for progressive taxation to ensure Government income covers something approaching the cost of its spending. Higher levels of public spending will require increased government income and more borrowing.
Social inequality is simply not affordable. This pandemic is in many ways a social disease hitting the disadvantaged harder. Billions have been lost by those least able to afford it while the more well off have accumulated savings during the pandemic. Can alleviating poverty be achieved without addressing the global problem of undeserved wealth? I don’t think so.
The time for a more significant green revolution which might prevent far more painful catastrophes coming our way in the next few years and decades. Progress remains too slow despite more “world beating” headlines.
The bottom line is that we need to spend more on the public sector. However bitter a pill that might be for politicians brought up in the Thatcher mould of life without a society, it is an inevitable conclusion of the pandemic. Unless we get this investment in place in the next few years, the next few decades will bring changes which COVID19 demonstrates we are not ready for.
So there are benefits in lockdowns and lots of costs too. Once the vaccines are delivered and the restrictions lifted, then we will need to think hard about the new society. COVID19 has demonstrated the old one was broken.


Good stuff as always – but I fear it will take more than a mere pandemic or two to change the mindset of all those orthodox Conservatives who think Britain deserves to be Great, foreigners *are* basically inferior (not that we're racist!) and that supporting the populace just because they are citizens is fundamentally immoral. Or maybe I'm just a curmudgeonly old duffer these days.