SUMMARY
- The second wave of the COVID19 pandemic is now a reality
- Cases in the UK are climbing rapidly.
- We are learning more about immunity; antibody levels drop with time, but an outbreak on a fishing boat suggests they do prevent disease and second infections still seem rare.
- The herd immunity versus lockdown debate is a false dichotomy.
- The private sector driven Test and Trace system has failed and needs to be redesigned with primary and public health taking the lead role.
- The failure of testing and tracing means that more lockdowns are now inevitable – they also offer an opportunity to redesign FTTIS (Find, Test, Trace, Isolate, Support.
- Our experience of COVID19 has meaning
Introduction
With winter some way off, COVID19 is extending its grip on society here and around the world. Despite evidence of immunity being more widespread than we think, there remain enough susceptible and vulnerable people around, enough poverty, enough malnourished and Vitamin D depleted individuals, enough polluted and crowded cities, and enough hyper-mobility for it to flourish once again on its accidental patch to temporary global dominance.
One day it will all be over and the final graphs of its rise and fall will be drawn, but right now we are in our own big moment in history and a pivotal moment for humanity.
This tiny virus may have a big say, perhaps even be the deciding factor in the US elections with seasonal increases in American cases, hospital admissions and deaths highlighting the incompetence of Trump with an issue whose immediacy he cannot, unlike climate change, and the other multitude problems of society, evade, postpone or deny.
Over here the sad news that deaths are running at about 300 a day; once again I am glued to the news, anticipating further lockdowns, restrictions, full hospitals, personal suffering and tragedy for many individuals and their families.
So is there any hope in this gloom? I think there is.
What is C19 up to?
Lots of amazing work is going o to try to define our predicament. The ONS community study of infections looks at rates of positive throat swabs and suggests that 430,000 people in England had COVID19 in the week of the 10th-16th Oct. The Kings symptoms tracker suggests slightly less at that time, increasing to 541,000 with COVID19 symptoms now. Imperial Colleges REACT project estimates 100,000 new infections daily. The actual number of course, is not known but will clearly be in that region and increasing. Neither of the estimates include children, so cases might well be more widespread than we think.
Nearly two weeks down the line from the ONS estimate, we see about 1,000 daily admissions which equates to a chance of being admitted due to the illness of about 1.6%. Bear in mind too that at this time of the year there are the other 15-16,000 daily emergency admissions to deal with in a health service for which pre-COVID winter was already a continual cyclical crisis.
It’s hardly a surprise that hospitals in hot spots are struggling to cope. It is harder to establish the risk of death due to the delay of about two weeks between admission, death and its notification, but clearly this is stratified by age and where you sit in our pathologically divided society.
Perhaps hospital admissions are the best measure of what is happening. These are easy to quantify and relate to day to day reality. As the shape of the curve evolves over the next week or so, we shall be able to predict the future with a little more confidence. Although the average of death is over 80, the average age of hospital admissions is 58.
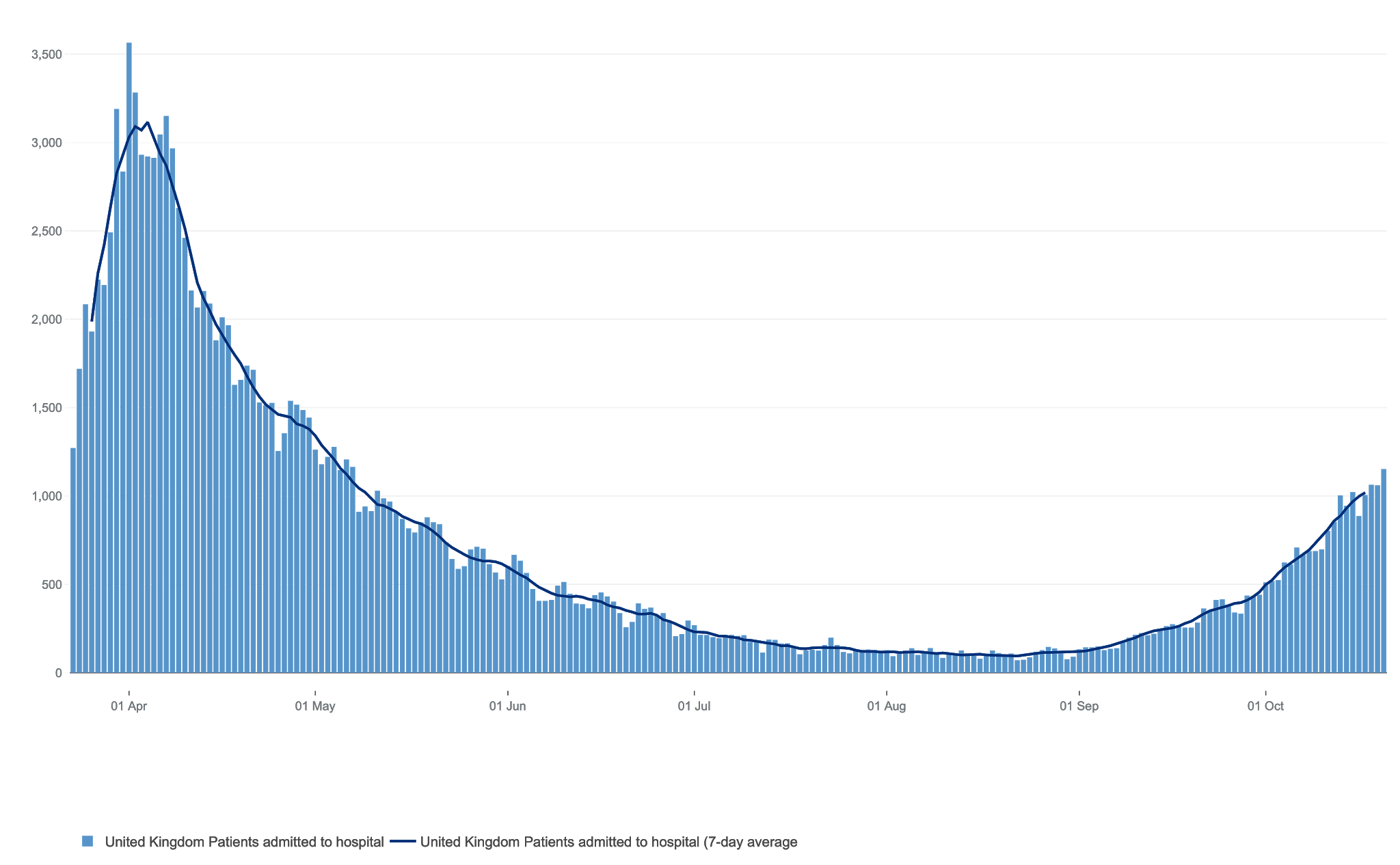 |
| UK hospital admissions – A longer lesser winter wave? |
It seems almost optimistic to hope for a lesser, but inevitably longer longer winter wave. The scientists are rightly concerned that we might have a much bigger longer wave with all the implications that brings for the winter and our future. I did wonder if the curve is beginning to flatten already, but I think that might be hope over expectation. We shall shortly see.
Why do waves end?
The graph below displays how seasonality is common to most viruses. The spring wave might well have been the tail end of COVID19’s natural winter history. I hope not. On the other hand, that wave will have spread immunity in the hardest hit areas, London, from which many will now benefit.
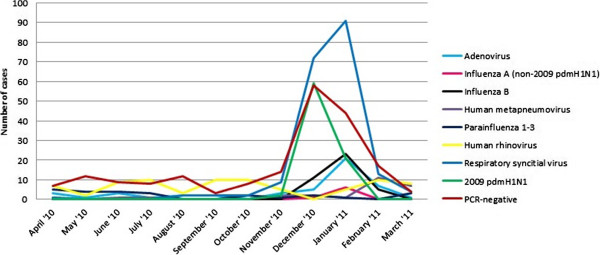 |
| Seasonality of viral infections |
Temperature and humidity levels played a part, as did the restrictions, but the second wave has come along with terrible predictability. I’m convinced that Vitamin D plays a key role in this seasonality, and despite the governments reluctance, could potentially be playing a big role.
It is not inconceivable that population wide supplementation with 4-5000iu daily would have a dramatic effect in reducing infections and their severity. A few politicians have taken up this cause and there seem chinks in the armour of the Department of Health. Despite the uncertainty, it’s definitely an opportunity being missed right now.
Predictions are notoriously difficult – remember the Imperial predictions of 500,000 deaths which drove our laggard politicians to take action back in March? Out by a factor of 10. There are plenty of gloomy predictions around once again and the numbers just keep rising.
Whatever happens, its clear COVID19’s success lies in its transmissibility and a long pre-symptomatic, or even asymptomatic phase under which is can covertly spread. Simple measures of distancing and hygiene really do work and masks too will become ever more a feature of day to day life. This really is a new normal.
Immunity
Gloom too accompanied a recent publication from Imperial Colleges REACT study. This surveys antibody positivity in over 100,000 randomly selected people and has been repeated three times now. The reductions in immunity they detected made headlines and might seem like bleak news, but hardly unexpected and not by any means the end of the world. Why?
For one thing, immunity seemed to be maintained in 74.5% of participants across three summer months.
 |
| Antibodies |
Positive antibody tests, according the dipstick method they use, dropped from an average of 6%, to 4.4%. Expectedly, older people had greater falls in positive antibody tests(40%) as compared to the young (15%).
Another problem is that the test is novel and might miss not be as accurate as we would like. It also, like a pregnancy test, gives a Yes/No result; so might mean that those with low levels of antibody are missed. Saliva tests, which more accurately reflect blood levels of antibody, are more encouraging with direct measurements detecting no decline in immunity over three months.
There is more to the story of immunity that what we can, currently at least, measure. White blood cells called B cells can remember the antigens of the virus and when encountered once again, rapidly turn into plasma cells which have the ability to churn out anti-COVID19 antibodies.
Don’t forget T cells which can also kill the virus directly when encountered. These are hard to measure in any bulk and so we cannot quantify their contribution to immunity in the population, but the science continues to be encouraging. There are, however, plenty of susceptible people out there for the virus to spread and R0 numbers heading towards their natural levels means we are not anywhere near herd immunity as yet.
One bottom line is how many people are getting reinfected? Thankfully so far his seems rare, which can only mean that protection does exist, even though it can’t be taken for granted.
Fishy business
An outbreak on an Irish fishing vessel provides an interesting case study of COVID infectivity and immunity. The crew members were extensively screened and all well before departure, with 3 members having positive antibody tests, indicating prior infection.
 |
| Thanks COVID! |
Swabs gave the crew the all clear, but nonetheless 104 of the 122 crew developed the infection while at sea, according to results back on shore after their fishing trip, giving an attack rate of 85%.
The three with measurable antibodies to COVID19 were fine. Despite the lack of information on symptoms and outcome, this hints at the usefulness of prior infection and that antibodies as we measure them do offer immunity. 15 of the others without antibodies but with very close contact with infected crew mates somehow escaped infection; perhaps they had T Cell based immunity which protected them, or just perhaps they were lucky.
This tiny snapshot of a well defined outbreak gives hints that the virus is very infective, antibodies work, and there may be other aspects of immunity at play. With small numbers, it’s interesting but speculative.
Vaccines
These remain much in the news with reports of the Oxford vaccine inducing useful responses in the elderly, but they remain some time away from roll out. The reductions in antibody levels reported by Imperial, if correct, might have implications for vaccines but are not the end of the world. It may well be the vaccines will be finely tuned to elicit a stronger immune reaction than ‘wild’ infections, many of which will be mild and not evoke an antibody response at all.
Trumps US Operation Warp Speed, (I kid you not) promises a vaccine this year, but this belies the reality of vaccine trials and development, indeed the first vaccine past the post will not necessarily be the best vaccine. If it not, then it may well be worse than no vaccine and it makes more sense to wait for the vaccine with the best trial results and least side effects before rolling them out globally.
The endpoint of the Oxford vaccine trial, it has been pointed out, is not even next year. By the time they are available, we will know a great deal more about where we are. The second wave will be behind us – by next April.
Barrington’s versus Snow’s.
These declarations take an opposite view on how to manage the pandemic. The former hopes for herd immunity by rapid viral spread in the less vulnerable with protection of vulnerable groups leading to less economic and social damage. Snow calls for a cautious approach based on the best science and maintaining the ability of the health sector to cope by restrictions and lockdowns if needed.
Differentiating them perhaps is their hosting. The “Great” Barrington Declaration platform is hosted by a US right wing think-tank and the John Snow response in the Lancet. Im always suspicious of the word “Great” being used for anything nowadays, be it Britain, or what to make America, again. Im with the Snow’s, much as I wish the Barrington’s were right.
The immense impact of the pandemic on the economy and culture are unmissable, but the single factor driving policy is the level of hospital admissions and the imperative not to overload the NHS.
Any reading of the history of pandemics reveal the situation if hospitals cannot cope. For the 1918 pandemic, the problem was that the undertakers could not cope, and the operational problem in the Black Death was simply how to bury the corpses. We live in modern times and are lucky this pandemic is a mild infection for most, but what happens if hospital services are overloaded is an issue not addressed by the ‘let it rip’ brigade.
Barrington’s are also guilty of suggesting that the vulnerable are a discrete manageable group. They are light on detail about how to isolate the poor, those in crowded accommodation, the elderly, those with other illnesses, as well as members of the BAME community. The vulnerable in the UK number over 10 million, many of whom have important roles to play in all sectors of the family our culture and out economy.
Nonetheless it seems the Barrington’s are winning, though not for long. Restrictions right now are piecemeal and complex, and nowhere near the lockdowns called for by those favouring the Snow view. The sad thing is that with nowhere really in control of viral spread it may even be too late, apart from that is, China and Korea, who got it right first time. Early complete lockdowns work. A short lockdown works if in place early.
For now, BoJo and his team are sticking to their guns to the frustration of the scientists. This will change as hospital beds fill up and more severe lockdowns become inevitable. A number of circuit breakers (or longer) through the winter seem to be coming, and once again we can lament in the knowledge that the later they are used, the less effective they will become.
Of course here in Devon, paradoxically it might seem, containment is still potentially possible though testing and tracing, but as a recent local experience without system shows, (see below) this is unlikely to happen, and our current low levels of immunity means the first wave, down here in the South West, is yet to arrive.
What to do?
Get healthy – Get as fit and healthy as possible, lose any excess weight, do what exercise you can, eat good food and in particular supplement with Vitamin D. Anyone smoking or vaping needs to consider the risks and enter the wonderful world of non smoking. This is now a matter of urgency. But what should we do as a society?
Testing Tracing Isolation Support: This is the bedrock of pandemic control. Our current system is only reaching 62% of contacts of those testing positive, well below the 80% estimated to be needed. Further, small numbers (11%) of people are isolating correctly and support is clearly not enough. Arrangements for isolation of cases in crowded households are not in place.
We have wasted the opportunity of the summer to design an effective system. Ignoring the potential to use primary care and public health teams to Find, Test, Trace, Isolate and Support has been a catastrophic error. In reality we have not used the NHS to do this job and are now paying the price.
Putting this right now will help with a third wave and mitigate the second, but the outsourcing of this vital task to the private sector has demonstrated the weakness of Conservative thinking and perhaps signal a new age where public services again take the lead role. This political failure could hardly be more vivid. Is the end of Conservatism as we have know it?
A recent case highlights the issue with testing. A friend with a child with relevant symptoms called 111 which led to advice to go to a testing centre. On arrival they were told the staff there were not trained to do the test on a child, but Dad could have a go! He tried half a dozen time before the swab was accepted. Two days later they were notified that the swab was inadequate and needed repeating.

Off they went again and repeated the testing, done again by Dad. The testing centre advised that they go to the paediatric department of the local hospital where staff would be trained to do the swab (bringing a potential infection into the hospital) but Dad persisted with the DIY swab. Two days later the test came back negative.
If the tests were being organised by local experts, this would not have happened. It seems the current set up cannot test children. Farce is a reasonable term to apply to this experience, and if the test was positive then testing and tracing would be that more difficult and less effective.
Now it seems, government have procured saliva tests in the hope of testing 10 million people a week, not quite the ambition of Moonshot, (which has been dropped) but in that direction. Some directors of Public Health have already stated that it is not all about testing, that the tests are not fully validated and if 10,000,000 tests are done with a specificity of 99% (unlikely) them 10,000 people a week will be isolating unnecessarily. There are all sorts of issues with the likelihood of dogma driven mistakes being repeated.
So, that having failed, what is the next option?
Lockdowns; Perhaps now is the time for a national lockdown of a fortnight? The longer it is left, the longer it will need to be. This could reduce spread of the virus and flatten the various curves of hospital admissions and deaths, but also offer time to completely redesign our failed Testing and Tracing system which lies at the heart of tackling pandemics and at our failure to contain it.
Areas, like mine in the South West, with low but growing rates would benefit from this, shifting infections further into winter. Alas, Im beginning to see little choice.
COVID19 has a meaning.
In some ways my post-war generation has had it lucky. We have missed the horrors of war at home, the Great Depression, grinding industrial poverty, and miserable infections of the past. But now we are facing our own difficult age in which COVID19 is a symptom of what is to come.
The ultimate cause of the pandemic lies in a total disregard of the importance of the natural world. We now are acutely aware of the dangers lurking in the blood of monkeys and poo of bats and can no longer afford to ignore the critical importance of looking after and expanding these remnants of the natural world.
It is a pandemic caused by poorly regulated commerce and capitalism, spread by a irresponsible travel industry and impacting on divided unequal societies whose weaknesses are now shown in sharp relief. Global organisations are needed to regulate them. Perhaps this will end the immature nationalism of Trump Bolsonaro and Brexit?
In terms of our organisation and collective effort, our failure to control it is the consequence of pathological, outdated politics. A belief in the power of technology and the private sector which now lie in tatters. The destruction of local government and many other local institutions also have weakened our ability to respond.
The dishing out of contracts to private companies who subcontract out work to others is little less than systemic corruption at the heart of government. In terms of those vulnerable to its ravages, it is a disease of society.
 |
| Let them eat sausages. |
Pandemic proofing
We desperately need more regulation to harness the capability of out of control corporations and business, particularly in the food sector. Cancelling Brexit would help, unless we lead the world back to restorative farming which seems unlikely.
Devolution of power back to local authorities and the ability to raise taxes to local levels would lead to stronger public health teams able to Find, Test, Trace, Isolate and support where it matters. This is beginning to happen and is now urgent.
A universal basic income for all citizens equating to the Job Seekers Allowance, would end poverty as we have know it and is affordable.
Local systems of food supply with healthy good at its heart is essential for any sustainable future. We need cities designed for people not cars and a transformation of our old polluting transport system away from car ownership and towards readily available electric taxis buses coaches and trains for journeys that cannot be done by bike or on foot. All this would have meant a healthier population and far less impact from the pandemic.
COVID19 has revealed that poverty, social inequality, polluted living spaces, low quality food and the indoor life can reasonably be seen as unaffordable as well as having been unnecessary, immoral and plain wrong for so long.
We need less wealth and less poverty – perhaps in a less unhealthy, unequal, society, there would be no need for a lockdown.
If the lessons we learn from this pandemic are put into practice, then COVID19 could in the longer terms save lives. Pandemic proofing societies would lead to a better world.