March, the peak last time, is six long months away. The impact on hospitals is already evident in hot spots and whatever scientists, politicians and pundits are saying, they are the front line.
My cloudy crystal ball is unable to detect whether the uptick is a the early ascending tail of a much bigger, far more threatening winter wave, or the beginning of an expected ripple. Plan for the former, hope for the latter.
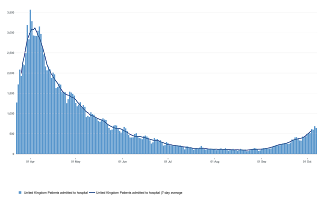 |
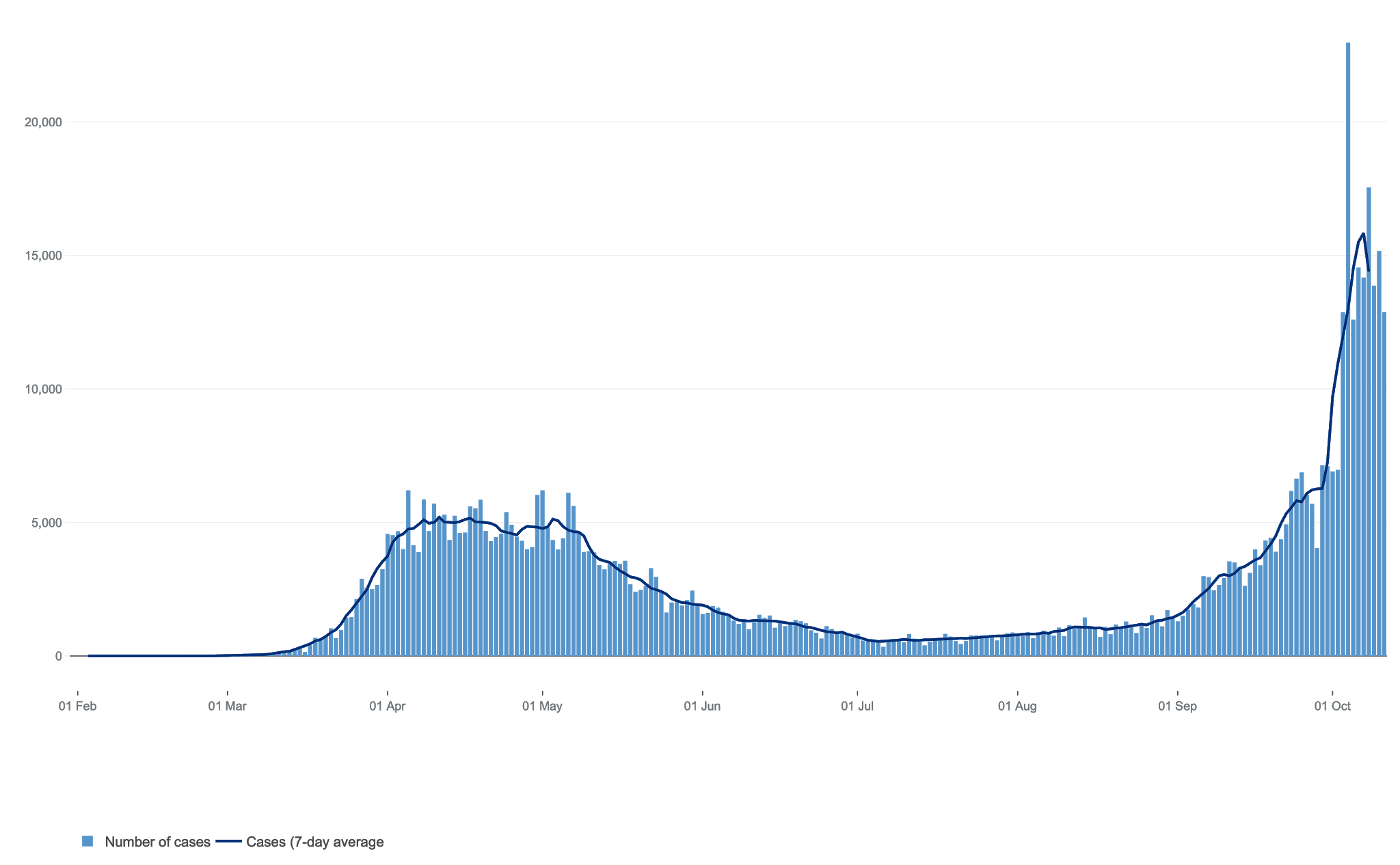
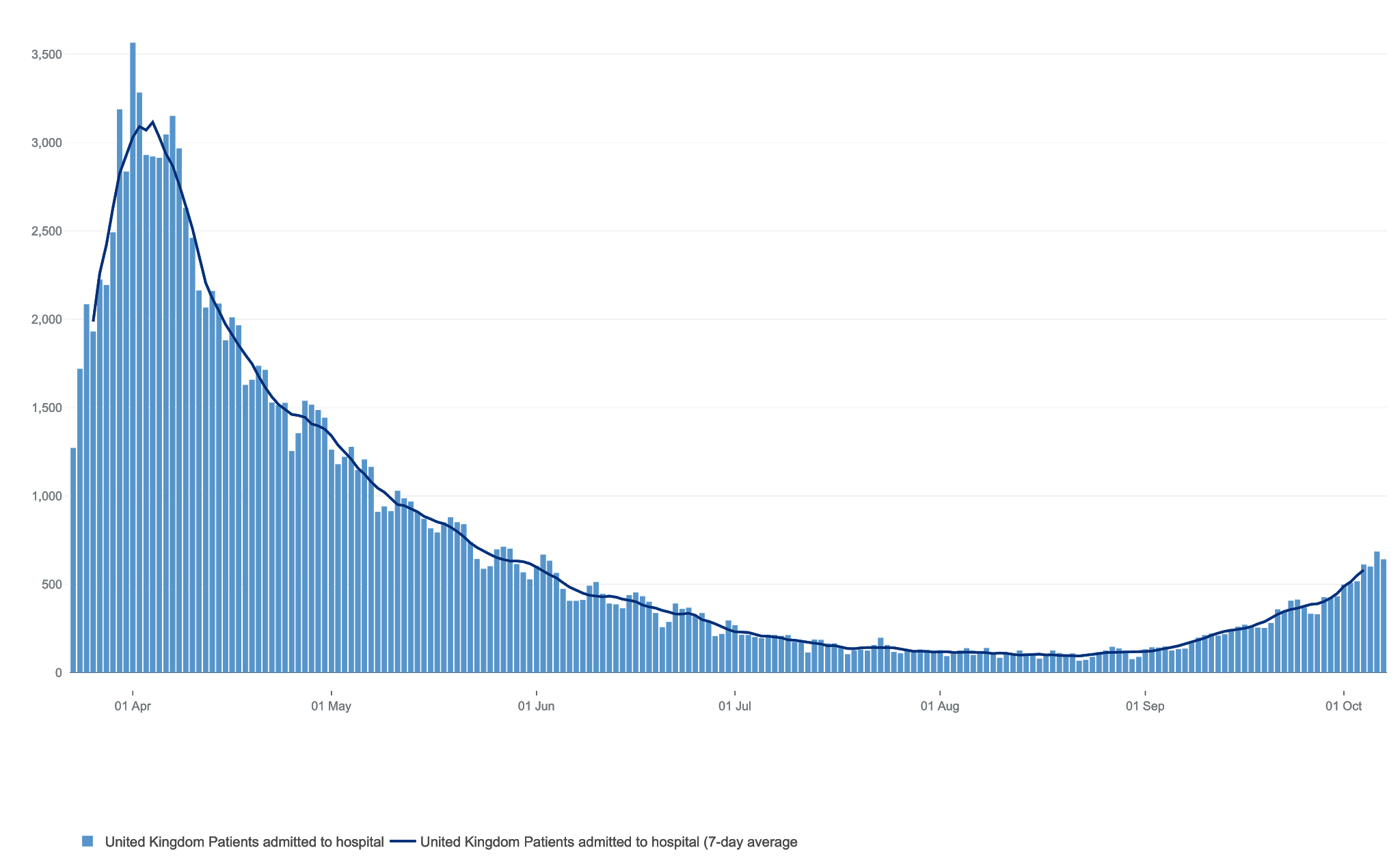
| HOSPITAL ADMISSIONS CLIMBING |
Either way, it’s clear that we are heading for very difficult times, both in terms of health impacts, so easy to quantify and understand if not to deal with, but also the mind bogglingly complex economic and social effects, some as novel as the virus itself.
As a doctor helping patients face life changing moments, and with my own diagnosis of MS, the hardest thing is that unnerving feeling of deep seated uncertainly. Individually, once you get through the treadmill of investigations to arrive at a clear diagnosis, then the fog can clear and for better or worse, understanding can mitigate fear and lead to acceptance. We can start to live with our diagnosis and adapt to it. Uncertainty is now a feature of daily life for us all.
With COVID19, essentially a disease of society, divisions among scientists and politicians have led to confusion and increased uncertainty in the population at large. In the US concern about COVID19 is mainly determined by political leaning, or vice versa. We follow these trends – to some degree it’s almost like Brexit all over again with a “libertarian right” tendency tending to want to carry on as normal and take the pandemic hit, to the cautious “humanitarian left” who want to preserve life at all costs. Individual freedom versus collective responsibility. They both have their points.
 |
| New Zealand1 – COVID 0 |
There is agreement that we have to give up ideas of ‘defeating’ the virus as they seem to have in NZ, where a crowd of 31,000 attended the draw between with their Aussie rivals
Up here in Europe, things have not gone so well, here, and in most of the world, it’s about containment and mitigation – we truly are in the COVID world.
So will have to learn to “live with the virus”, but what does this actually mean?
Living with the virus – the “medical” view:
The harsh advice coming from the Chief Medial Office and SAGE might seem to come from a narrow medical standpoint. Critics say that it fails to take account the economic impact and significant collateral damage done by restrictions which dampen down viral spread so dependent of human contact, but also destroy quality (and quantity) of life for many, damage education as well as the unprecedented costs cash cash costs of lockdown.
 |
| SAGE – Sagacious? |
It is driven by a desire to prevent illness and death, but also ensuring a functional NHS. The graph of hospital admissions above represents a national picture, but in Liverpool, and other Northern towns the number of cases is twenty times (600/100000) that of West Devon (36) from where I write.
In cities, it seems, the virus is spreading rapidly, and already stretched local services can become easily overwhelmed despite less worrying national stats. This is simply unimaginable in peacetime. Neither is it simply a matter of shipping patients from one area to another – this can be done, but holds big risks for all.
Being unable to access health care in an emergency is something my generation, uniquely, has never experienced or even contemplated.
For anyone working in the NHS these are scary times. 620 frontline staff have already died. Even though much has been learnt from the first wave, the NHS was already stretched to breaking point before the crisis and now has to deal with a triple whammy of COVID19 cases, the reduced efficiency associated with distancing as well as the catching up the host of other illnesses knocking at the NHS’s door.
Seen like this of course, everything must be done to reduce the spread, slow down the virus and “save the NHS”. So Chris Whitty is full of foreboding, hinting at the significant restrictions on their way, miffed that they are not in place already.
His advice is that we need lockdowns, circuit breakers, and restrictions until the R0 is below 1 and then we can all go about our business until the R0 number goes above 1 and then repeat the cycle.
Keir Starmer now agrees with a 2-3 week national lockdown – but how many times this winter will this be needed? Clearly if you are going to do this then the earlier its done the more effective it will be – perhaps it’s a bit late already.
This cycle continues till through the winter. until the whole thing is over, whenever that might be. A vaccine would help, but is not going to make much difference this winter and there are emerging issues of effectiveness, safety and compliance. Perhaps by next winter a vaccine will be ready, but even that is not clear cut
In a way, that is the pure epidemiological view of living with the virus.
Living with the virus – the “economic” view
The recent support for those made redundant by the restrictions makes for sober reflection. The Chancellor will pay a poverty generating 60% of income to those affected by COVID related redundancies. Early estimates suggest a cost of £100 billion a month – for 6 months. That equates to £30,000 per family in the UK in addition to the resources already spent. It is hardly surprising that we coming to a point when we have to ask -is this simply unaffordable?
The Barrington Declaration seems to sum this up. This group of respected scientists have, for reasons I fail to understand, allied with a right leaning Koch Brothers funded American think-tank to deliver the most simple of messages – simply let everyone get on with their lives apart from those at risk who should be protected thoroughly.
Wonderfully simple. Easy to buy into and headline generating. It is right that this must be debated. There are however, holes in their argument which are not clearly articulated in the declaration.
For instance, the Americans are already having a bad time.Their first wave was followed by a very thick “tail” with about 1000 deaths a day through the summer and now have more than 200,000 total deaths heading into the winter. They are really still in their first wave. This suggests the winter will be very tough for Americans. Their patchwork chaos of response, confused federal thinking, and poor population health have left them precarious, weak, vulnerable. Not qualities Trumpian Americans (Trumpists??) like to shout from the rooftops.
The “vulnerable” include the BAME community, the overweight, those with metabolic poisoning from the typical US drive “western” diet, and of course, those over 65. So those vulnerable are actually quite a large group to try to isolate. 30% of Americans are obese. In my surgery, diabetes had become ever more common, with 5% of people diagnosed and many others in a diet induced, “pre-diabetic” phase which also seems to fuel vulnerability to COVID19.
The “vulnerable” are also parents, grandparents, carers, key workers, teachers, politicians this list could go on – simply stripping them out of society is difficult. What about the vulnerable living in crowded housing? Those in care home rely on visits of loved ones for quality of life.
They also fail to quantify the deaths in the young, (increasing in the US) in care workers, in the developing nations, and forever quote the average age of death as the foundation for “back to normal” approach.
This focus on death fails to consider the effects and costs of those who do not die, or sometimes even go to hospital. Sick leave, strained public services as well as the long term effects of COVID19, which are sadly far more common that we thought mean that the impact on society goes beyond the death and hospital statistics.
So although in the declaration is attractive, hinting at a straightforward solution to the problem, it has been criticised for its inability to actually look at what is happening on the ground. The infrastructure needed to isolate so many people suggests a social and political transformation which is not on anyones lips.
We can’t have everything
What is self evident is that we cannot have our cake and eat it. We simply cannot have an economy which can function as is has in the past, a COVID19 pandemic kept in its box, and hospitals just ticking along their normal edge of the cliff.
At some point a balance will have to be struck between the competing demands of preserving life and livelihoods.
This is not easy. COVID19 is a nasty illness. Think of flu, but about four times worse. Some people think thats not as bad as it really is but for significant chunks of the population it is life threatening. Then there is the suffering of patients and the intolerable demands on care staff to think about as well as the emerging long COVID to consider. These cannot be ignored.
Middle ground?
I cant help but feel that there is some middle ground;
The young. Surely we do everything to keep schools and universities open and functioning with young people allowed to mix in larger bubbles reflecting their normal scholastic life. The social aspects of education are critically important for the development of life skills.
Sending a whole secondary year home because of one positive test is not practical and has led to significant reductions in education for up to 20% of UK school students as we speak and can only get worse with this policy in place. Stay at home is you have symptoms and take care of relatives might be better advice for school kids.
 |
| Plymouth University |
Isolating university students in their halls for on-line degrees without much personal input from academics and reducing the opportunities to meet the acquaintances, friends and develop social networks which define life for so many begs the question – what is the point of going at all?
University accountants must be having sleepless nights as they realise that pure on-line courses hints at the end of physical universities. On-line lectures can be ‘bought’ from Harvard as well as from Huddersfield. Put that into the COVID19 equation.
Perhaps Universities might head towards having giant bubbles including food, drink and social activity enclosed within a busy campus. Trips home could be sandwiched in between testing and those with symptoms isolated on site and supported with good food and on-line personal support.
It might seem selfish to put what might be seen as the hedonism of youngsters before the life of the elders, but the young are our future and their prospects are already compromised by many of the factors which have allowed the spread of the virus into their lives in the first place
If point of care testing comes along, if it does, then let’s consider students as a priority group.
The elderly in Care homes can be better protected, in particular with enhanced testing and any trials of rapid point of care testing focused on staff and residents to ensure their ongoing ability to function. Essentially homes should be kept COVID free. Here too, maintaining contact with families is essential and can be achieved with visiting rooms as well as novel electronic means.
This all needs funding. De-fragmention of the care home system would help, but as a sector we have to try to make do with the privatised, publicly funded chaos from thousands of independent providers who have to be brought together and enabled to stay free from COVID19. This is not an easy task.
The vulnerable: Perhaps our vulnerabilities might actually be started to be examined a bit more positively. Is is not impossible to lose weight, to take vitamin D, to stop smoking, to eat nutritious food, to enhance community, to strengthen local infrastructure, to beautify cities, to engage with politics. The majority of people the 4.8 million people living with type 2 diabetes can be cured with a healthy diet. Pandemic defining vulnerabilities can be slashed, but how many times have you heard this from the political briefings?
The illness itself. Nightingale style, or other dedicated hospitals could be useful to assess large numbers of people presenting in COVID19 hotspots as well as staging posts for the elderly to return to care homes, or to their own homes if crowded, with negative tests to ensure non-infectivity. Yet perhaps too we might have to admit that 100% success here is not likely and that there will be mistakes, infections and deaths. Hopefully not on the scale of the first wave.
COVID19 – An illness of Society
COVID in many ways is an illness of our society. Our collective health is poor and has been made poor by the politics which defines us. Food policy, air pollution, sedentary lifestyles, inequality and racism give the virus the fuel it needs. The lack of a sane food policy lies also at the pandemics origin in the dwindling habitats of China. We created the conditions for this virus to emerge and much of its subsequent pathogenicity.
With better designed cities, food policies based on good farming and nutrition, social and racial equality, employment based on wellbeing, we would be able to deal with the pandemic without a hint of lockdown or economic restrictions. That is why I say it is an illness of society.
The time has come for Universal Basic Income, a buffer which would increase flexibility, freedom and help in the modern age of part time working.
 |
Universal Basic Income
– the 21st Century
safety net! |
Our politicians seem adrift because they are. Decades, even centuries of misbehaviour are catching up with us and we in simple terms, have a society which is destroying itself.
It seems to me the “medical model” will work, but it will cost many many trillions of pounds which we have not got or are likely to earn.
The “economic model” will work, it will keep our economy ticking along like the bomb it is, but cost many lives and much morbidity we are not prepared to accept.
Perhaps an economy based on generating good health, environmental improvement and wellbeing might bring together both models – its time has arrived. Indeed, it’s now or never.
I





Thanks. It's a really interesting study and seems to avoid the reverse causation problem. (Disease causing low D3 levels) A recent bolus dose made a big difference. Bit of a mad way to supplement though. At this stage of the pandemic Im pretty convinced it makes sense to supplement with D3. Please do spread the word. Let's hope the bigger study planned in Cordoba doesn't take too long.
Thanks.
A study in Angers France has found a correlation between vitamin D and CV19 survival. The numbers in the no vit D group were low, so we are left again waiting for larger study
https://www.sciencedirect.com/science/article/pii/S096007602030296X
Thanks Colin – especially liked that last paragraph!