The days are shortening and the cool damp Autumn seems here rather prematurely as we leave behind another climate change altered damp squib of an August. Despite the resultant diminished harvest, COVID19 remains the headline story in every paper and every news bulletin just about daily.
We are entering a crucial phase of the pandemic, but will this next phase be a gigantic new terrifying wave, or just a demonstration that the pandemic is over?
What’s the score with COVID19?
“Cases” are rising everywhere and there is anticipation in the air. Schools are heading back next week in England and are already back in Scotland, this annual exodus is usually accompanied by a flurry of viral infections and a sigal that winter will be here soon and with it the threat of a second wave, though perhaps not; no one really knows for certain.
Right now there is lots of concern about the increasing number of positive tests, but what we do know is that people with COVID19 are not turning up at hospitals in any significant number and the number of deaths remains low.
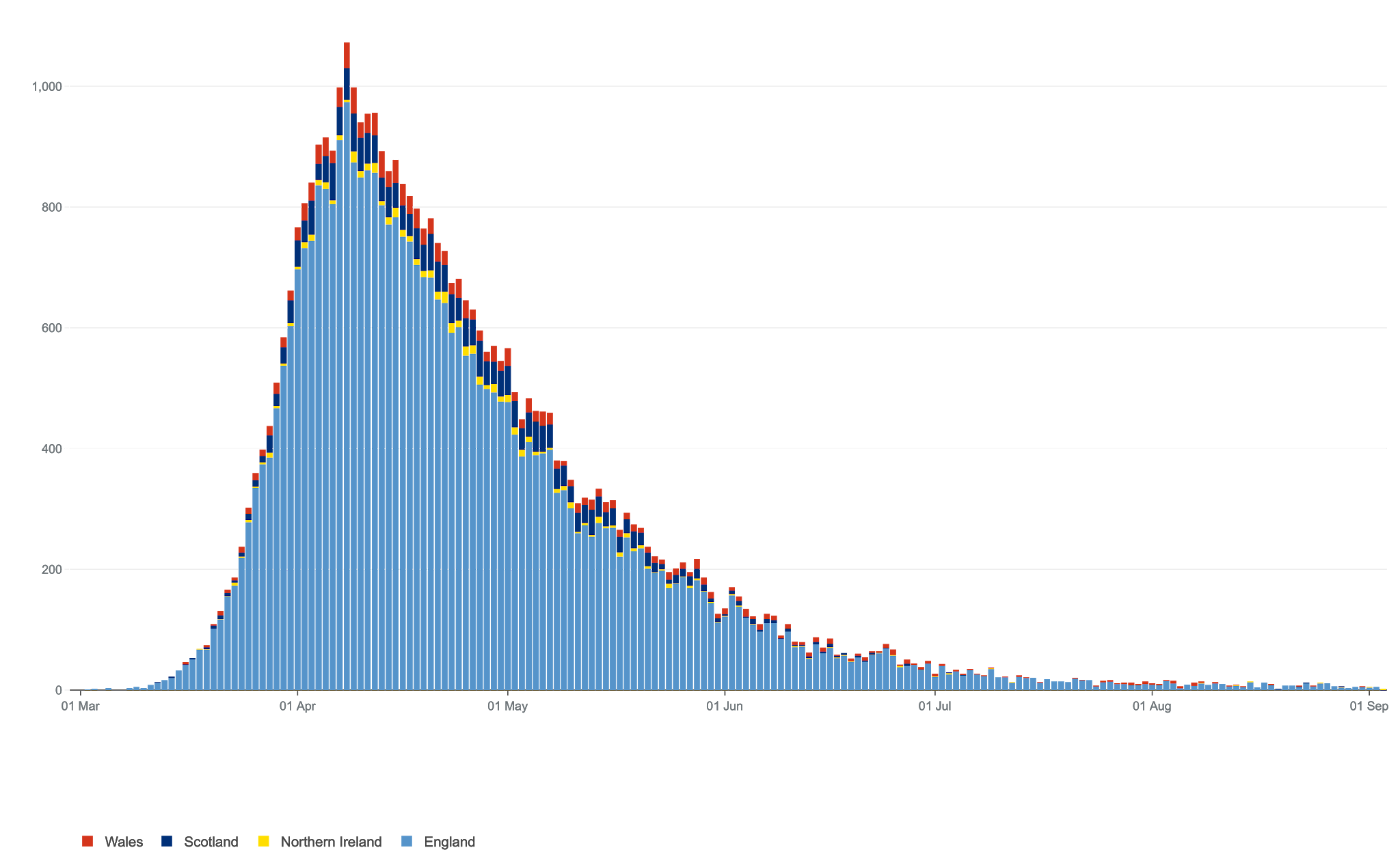 |
| UK COVID19 Deaths |
The graph on the left shows deaths from COVID19 in the UK. Despite the increase in what are incorrectly called ‘cases’ there is no upturn in the number of people arriving in hospital or dying.
So things right now are very different from spring. Those huge summer bank holiday day beach parties and other social gatherings have not led to any problems for the NHS or any demonstrable health problems to outweigh the health benefits of the fun had by participants.
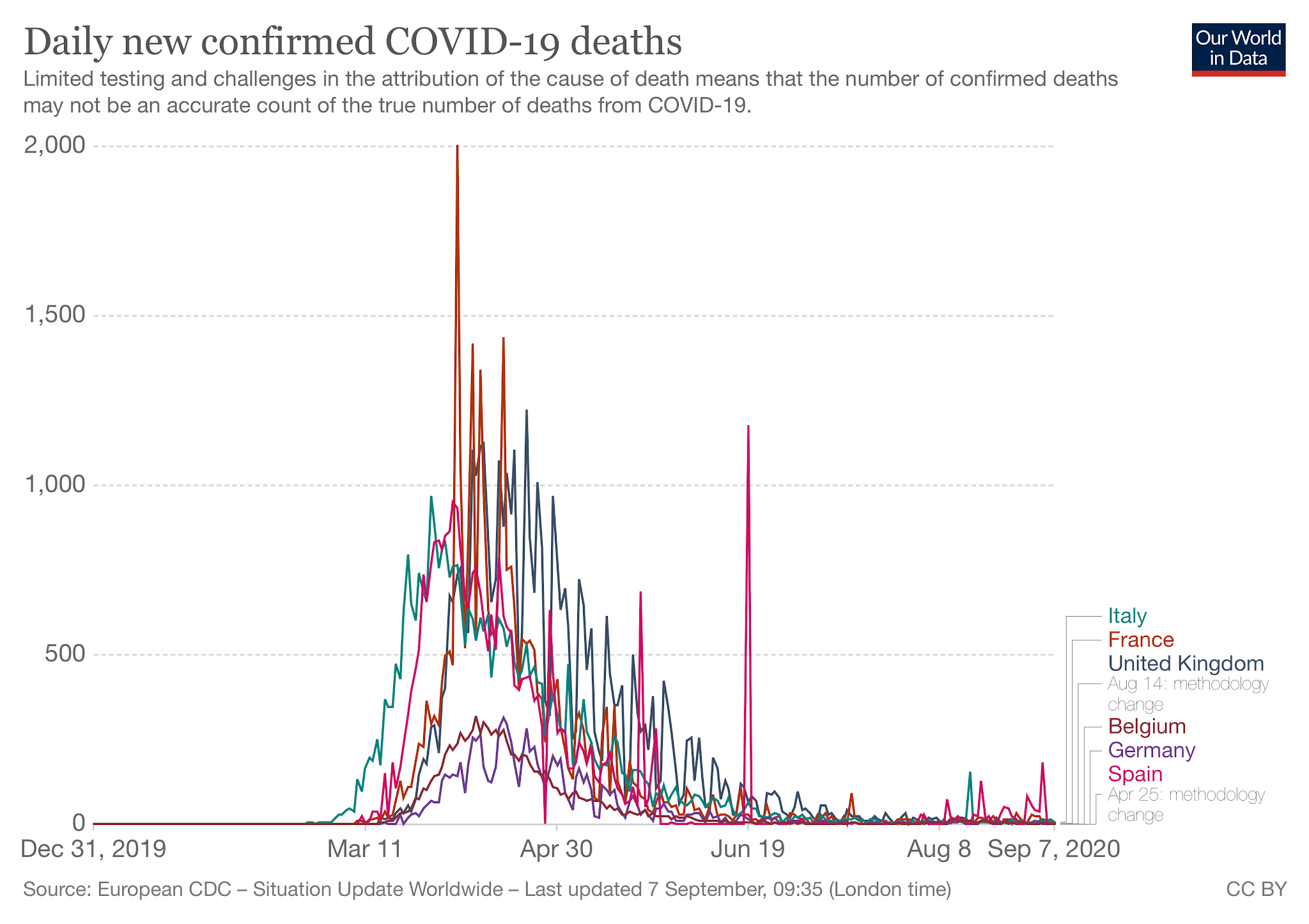 Around Europe the picture is repeated with no increase in mortality anywhere. so far. There has nonetheless been lots of worry in the news, local lockdowns, quarantines and ever more testing of people with and without symptoms. Matt “Handsfree” Hancock has even been talking up saliva tests which would enable us all to be tested every week and yet another app to trace our every move and contact. The project, appropriately enough, is called “Operation Moonshot”.
Around Europe the picture is repeated with no increase in mortality anywhere. so far. There has nonetheless been lots of worry in the news, local lockdowns, quarantines and ever more testing of people with and without symptoms. Matt “Handsfree” Hancock has even been talking up saliva tests which would enable us all to be tested every week and yet another app to trace our every move and contact. The project, appropriately enough, is called “Operation Moonshot”.
 |
| Just 3,999,999 to go then! (From Open Democracy) |
Once again most of the work is to be outsources to private sector chums Deloitte (revenue $43bn) in what has been called the biggest single act of privatisation ever. No change there.
Handsfree’s rhetoric is as usual way ahead of the technology available and seems designed to make a “world beating” headline rather than advance public health. It is also a gigantic shift in resources from the public purse to the private sector as well as missing the opportunity to get the NHS ready for the winter by building on locally based services already in place.
Yet, the plans are already being scaled back by the real world. They now plan to test 4 million people a day with a longer timeframe. The upshot of this is that more tests will come back as positive. There will be more infections detected, and they will be called “cases”. Confusion reigns!
Infections or cases – there’s a big difference
There is a fundamental problem going on with simple out-dated terminology which is having some major implications. This refers to the rather anodyne “case fatality” and “infection fatality” rates.
In past pandemics, such terminology made little difference. Historically, people with infections became ill and sought help. The case fatality rate (CFR) was simple to calculate; divide the number of deaths by the number of people turning up with infections (cases) and then multiply times 100. In March the CFR in the UK from COVID19 was 14% and has been falling fast ever since.
“Infection fatality rates” count anyone at all with the infection, including those with few or no symptoms. You may have to do more looking to count the people who had milder illnesses and didn’t seek help to know how bad the overall infection is. This will be of course, be lower than the case fatality rate. In COVID19, 10 times lower.
This is the first pandemic where we have been able to go out and test widely for infection among the general population and so the difference between the two measures are widening all the time. Infections appear to be rising everywhere, causing panic, yet clinical cases remain thankfully uncommon. Panic is entirely inappropriate. It is chalk and cheese.
In March, we were only testing people who were admitted to hospital, severe clinical cases, and the case fatality rate was 14%. Now we are testing 180,000 people a day and yet treating the resultant number of often clinically positives with the same sense of anxiety.
What we have really found is that the virus has continued its spread through the summer and is widespread in the community. This is no surprise at all as the young become active and the economy grinds back to normal, including 100 million state subsidised meals (how many of them will be adding to the obesity problem I wonder?).
So far, I am rather reassured by the apparent lack of impact of the virus in the summer despite the ongoing number of cases. ONS estimate that in the last week, there have been 27,000 people infected with COVID19 in the UK and there has been a total of 40 deaths. An infection fatality rate of 0.15%, that is 1 in 6,75.
Good news?
In this sense a higher level of infection coupled with a low case load is good news. It might mean that the virus is, or has become less virulent, that more people have developed immunity, that higher Vitamin D levels have had a positive effect, and that vulnerable and older people are continuing to shield.
It may also be that many people are getting infected with a lower viral load. That is, coming being infected with a small number of viruses by passing someone in the street or in a cafe and inhaling a small number of viruses, as opposed to trying to manage an unwell household member who is expelling millions of viruses with each cough.
Or a bit of all of this.
Or, that it is highly seasonal and we have not yet entered the difficult winter phase to come. We shall see, but such a high number of infections without much clinical impact has to be reassuring at this point in time.
If people infected develop immunity to the virus, either through the development of antibodies or memory T cells, they will also be contributing to herd immunity and will be protecting, in that sense, family members and others they are in contact with through the winter.
So let’s have another think about the logic behind this mammoth testing project?
What is testing and tracing for?
The test itself look for fragments of viral RNA and are able to pick up a single strand from a single virus, and so will tell you that you have had the infection, but will not necessarily tell you if you are infected, or infectious. It’s rather like a bank statement that just tells you that you have, or don’t have money in your account, not how much. All a bit blunderbuss really.
It means that if people with positive tests are traced and isolated, it will slow down the spread of the virus. This makes sense, but it is working?
In reality the virus continues to spreading very well despite the measures. This is hardly surprising given that it is very infections and most infections will come from household members, particularly in multi generational households and deprived areas which are taking the brunt of the resultant restrictions.
Testing will only work is the tracing is effective and people are financially supported to isolate for a fortnight. The recent £13/day uplift will not be enough if you need income on a day by day or week by week basis. You can apply for Universal credit as well as SSP – Im sure the form filling for all that will take up the whole two weeks!
Yes, even in poorer areas, with their increased rate of infections there is still no increase in cases, for now at least.
So might restrictions be following the wrong numbers? PCR tests should be the driver of the tracing strategy, wider restrictions decided on local impact on health.
To add to the problems, care homes continue to complain of ongoing delays to results for tests which will compromise the safety of some very vulnerable people. Add this to the list of problems not sorted out over the summer.
Lockdowns
Local lockdowns might be better designed to react to outbreaks of illness, when clinical disease is counted by calls to GP’s (still uncounted) or call centres, or hospital admissions. But they are being put in place simply according to the number of positive tests irrespective of why this has happened.
It’s reasonable to expect this will, as usual, impact on the most densely populated, more polluted and poorer communities which have already been hit hardest by the virus and its economic consequences. Insisting a member of a busy household stays at home for two weeks is a pretty good way to spread the infection to other household members and then to their contacts.
In these areas with high levels of zero hour and low paid workers unable to afford sick leave, it is hardly surprising they are more infected. The poorer are hit harder in every epidemic you might think of from Cholera to TB and Influenza, and in this country we have high and increasing levels of inequality
Perhaps “lockdown” might be better applied household by household, but the support is not there to allow this to happen and advice from distant tracers is easy to ignore.
It’s as if the politicians assume that we all have facilities like spare rooms and en-suite toilets and bathrooms to isolate at home. “I’m off to the East Wing for a fortnight darling – tell the butlers to leave the dinner by my door.”
Certainly if there is one situation where masks are useful, it is sharing a house with someone who is infectious.
So what is going to happen now?
Viruses are very unpredictable. Remember the impact of the terrible Zika virus in South America? Those infected mothers whose babies had small brains (microcephaly) – thankfully, and for poorly understood reasons, the virus changed its behaviour and no longer carries this threat. COVID19 might change too.
The case of a young man from Hong Kong with a second COVID19 infection made the news, and showed that his immune system had successfully kept the virus from causing any symptoms. There had been some changes in the proteins of the capsule signifying that this virus is capable of mutating too. The evolutionary pressure will be for illness to become milder as milder viruses spread more widely. Fingers crossed.
So there are reasons to be hopeful that we wont see a repeat of the spring. Yet, hospitals continue to have little spare capacity after a decade of cuts and our low level of provision of hospital beds, but have more experience with the illness and how to manage it.
With schools and soon universities back in business, an increase in infections is not just likely, but certain; yet how this translates into people who need help is uncertain. Perhaps there will be a middle way as an outcome for all these uncertainties. A smaller more manageable winter wave which will not swamp the NHS and so allow life to carry on till the next modern crisis.
As I write there has been an increase in positive tests to 3,000 or so a day for the last two days. If this rise is sustained as activity increases then the next few weeks will be telling. The positive tests are mainly in the young who deal with the infection well, but there are concerns it will spread to older, more vulnerable groups and then hospital admissions will rise, I have hopes this will not happen, we shall now see.
The alternative to allowing this to happen is to lockdown again, and there is a general agreement that this is not affordable or even possible, and indeed that it may not ever work. The lack of a locally based public health test and trace operation will be a big disadvantage as well as the lack of the financial support needed to ensure people testing positive are able to stay at home and isolate where they can, though this is not straightforward either.
I shall be wearing a mask in shops and following the rules, but now is the time to focus on health again. I shall post on Vitamin D shortly as more evidence has emerged regarding its usefulness and all those other measures to improve immunity.
Meanwhile…
I can’t but help reflect on the causes of the pandemic; agribusiness and destruction of

ecosystems where the planets remaining wildlife largely resides. Bad farming is behind this problem, and is continuing to foment the next spillover pandemic. Our forthcoming trade bills are unlikely to address this and more likely to make matters worse.
Brexit too is emerging from behind the scenes, being pushed on all the time by a prime minister whose competence is clearly lacking and is likely to be put out to grass before the brown stuff hits the fan. This is despite the pandemic clearly demonstrating the need for international co-operation and unity.
I sigh in frustration that this gigantic financial and administrative effort would be so more effectively targeted at the transformations needed in our society to adapt to climate change which as we speak is far, far more dangerous than COVID19.
Thanks again Colin! It seems to me, more and more, that bad maths and sloppy use of terminology produced models early on, that are wrong by a factor of ten. (that persky decimal point!). Roland B Brown and Dr Mark Kendrick have good explainers, too….
Thanks again Colin! It seems to me, more and more, that bad maths and sloppy use of terminology produced models early on, that are wrong by a factor of ten. (that persky decimal point!). Roland B Brown and Dr Mark Kendrick have good explainers, too….
Your quite right – thank you – Ive updated the post.
Dr B should
An infection fatality rate of 0.15%, that is 1 in 6,670.
read 667?