For me, the best April fool prank was the spaghetti tree harvest from the BBC in 1957. This Panorama ‘documentary’ highlighted bumper crops of spaghetti being picked from laden spaghetti trees by happy workers. It convinced a few and created a laugh for many.
Im beginning to wonder if the changes in pandemic management are another great hoax. Ending free testing, abolishing all public health measure, funding for world leading research drying up, and now a budget which promises tax cuts with little more than a nod to the cost of living emergency and an energy strategy that seems to have forgotten about COP26 promises and energy bills. All this and more leaves me with that April the 1st feeling. Sadly, none of it’s a joke.
Short COVID
As the significant problems of long COVID are becoming clear, there remains more “short covid” around than ever. The feeling that the pandemic is petering out is born out of reduced publicity, a casual approach by politicians as well as the ghastly war in the Ukraine distracting our attention from the pandemic’s daily toll.
In the last week of March there were more people in the UK known to have the infection than ever. Suggestions have been made by myself and others that now is the best time to get infected, due to a milder virus, the time of the year, and better treatments. This applies less with age, and vulnerability and does involve a toss of the coin as far as long Covid is concerned. For others, the ‘let it rip’ policy does mean that millions are infected every week. If nothing is done to limit spread, this is what happens.
The huge numbers do not account for those who are not testing, and those tests that are failing to pick up illness, so the reality is that right now the pandemic is rampant.
Thankfully treatments are better and immunity more widespread, though Paxlovid, probably the best, is scarce to say the least, and the more available Molnupiravir not really all that useful. While not preventing new infections, vaccines are making them milder for most people. This leaves us with plenty of problems for the elderly and vulnerable whose immunity wanes more quickly. Clapping and bashing pots and pans in gratitude to the NHS has given way to an assumption that the health sector is coping well, it’s really not.

Long waits in ambulances are a sure sign of a health system in crisis, but has sadly become the norm. A friend recently had to wait 14 hours in an ambulance before being seen as an emergency. If you call 999, bring a book to read!
The health sector is simply used to a state of continual crisis, exemplified by long waiting lists for elective surgery, unacceptable ambulance waits and problems getting to see GP’s. Staff shortages and recruitment are the norm. General practice, certainly in the cities, is in big trouble and in many places being taken over by American corporations and will morph into a salaried service with sessional doctors.

Takeover of primary care will lose the essential feature of seeing a doctor who you know and who knows you. For me that is very sad.
B2 wave
So as I write, a whopping 7.6% of people in England are infected with the latest variant of Omicron – B.2. The significant B.2 wave is causing 2,000 hospital admissions and 200 deaths a day. Although 25% of COVID patients have testing positive after admission, for many that does not mean the admission is incidental.
For example, someone admitted with a stroke and then testing positive falls into this category – the risk of stroke, and many other problems leading to admission, are significantly increase by COVID. Given a prevalence of infection in the community of 7.6%, it might be expected that about this number of admissions would be truly incidental, but the majority will be due to COVID and its many impacts on health.
My local hospital, for instance has admitted 166 patients with COVID19 in the last week, which gives the 400,000 people in its catchment area locals a very low chance of being admitted, and thus it is easy to disconnect from the unprecedented pressure on the services we tend to take for granted, until they are needed.

For some, the B.2. symptoms can be more like a cold with runny nose, headache and sore throat. The vulnerable continue to be at risk.
Other than admissions, schools, the heath sector and businesses are being harmed by staff absences, giving the lie to removal of public health measures being good for the economy. Add to that the human and economic impact of Long COVID is a growing problem and likely to rise as cases increase. Air flights are being cancelled due to COVID problems of staff. Even if we have reached the peak of this latest wave, hospital admissions will continue to increase for a few weeks yet and who know when the next variant will take off. Living with COVID will be tough.
The dirty man of Europe – again!
The UK earned the unwanted title of “The Dirty Man of Europe”, some time ago. After Brexit it sadly applies once again to pollution control and laissez-faire attitudes come at a cost with infection too. We could easily do better. A friend recently travelled to Italy where the wearing of decent masks (N95) is widespread, Green Passes to prove immunity are still needed to access public areas and testing is widespread.

Perhaps masks, like in the Venice Festival, are more culturally acceptable in Italy. Or perhaps they are just more sensible.
I know simple comparators are tricky, but does this hint at the risks we are taking? The chancellor might baulk at the ongoing costs of the pandemic, but needless staff absences and problems with business and public services hint that penny pinching costs more than investment.
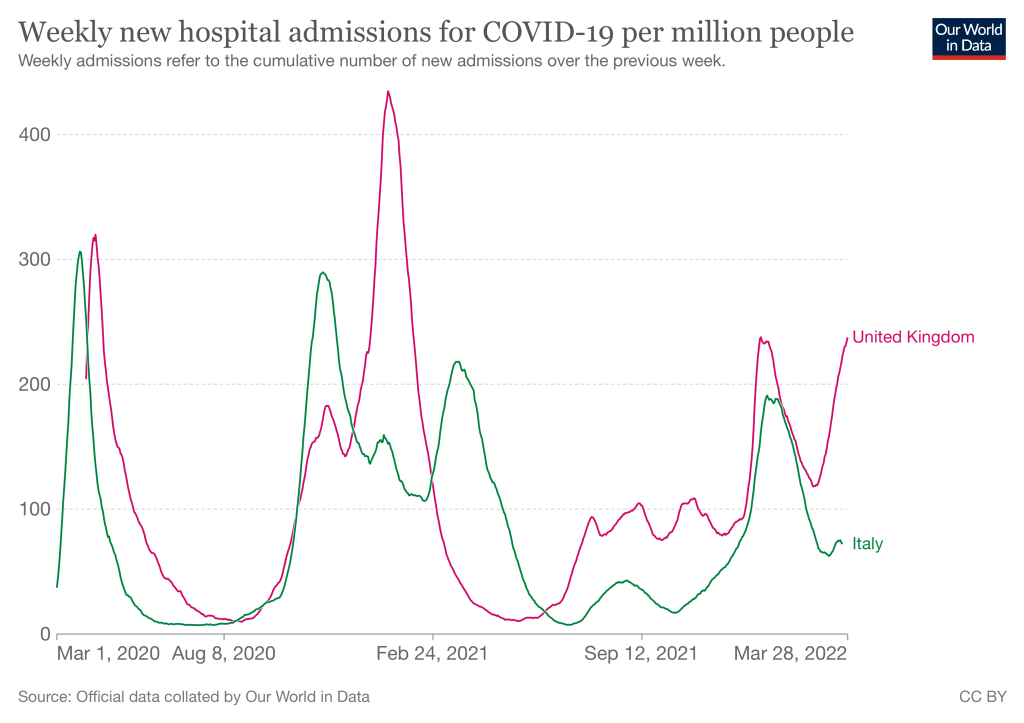
The B.2 wave is worse in the UK where we have abandoned public health measures and are now ending free testing.
Crystal ball time
Arguments still go on as to what will happen next. You can’t wish away hospital admissions and deaths by stopping testing, even if means the number of ‘cases’ will fall. Unlike influenza, COVID19 has yet to become seasonal and public health measures might have to be dusted off.
There is hope that new variants will continue to be less severe, but viral success depends on transmissibility with much transmission taking place before symptoms and so the severity of the illness matters less to viral evolution. As I have pointed out before, perhaps the milder common cold coronaviruses have evolved from more severe variants (Russian Flu?), and maybe transmission to and then from animals like deer and mice with high levels of ACE2 receptors will drive evolution in a milder direction. To some degree this is my wishful thinking, we don’t really know. Again, I’m keeping my fingers crossed.
What we certainly need are better vaccines as the present ones are getting rather dated. I hope these will be ready for the autumn. Lurking in the back of my mind are the consequences of a more serious variant and how that might impact on our society indeed species and if we can afford another global crisis to add to our multi-crisis world. Vaccines need to be at the ready.
Ivermectin – flogging a dead horse
Another well conducted trial adds to the others which show that Ivermectin is not useful for COVID19. I wonder how much more research money will be wasted flogging this long dead horse. It’s no longer a matter for medicine, but politics with understandable but indiscriminate anti-authoritarian attitudes meaning that the Ivermectin fans will not let go.
Levelling down
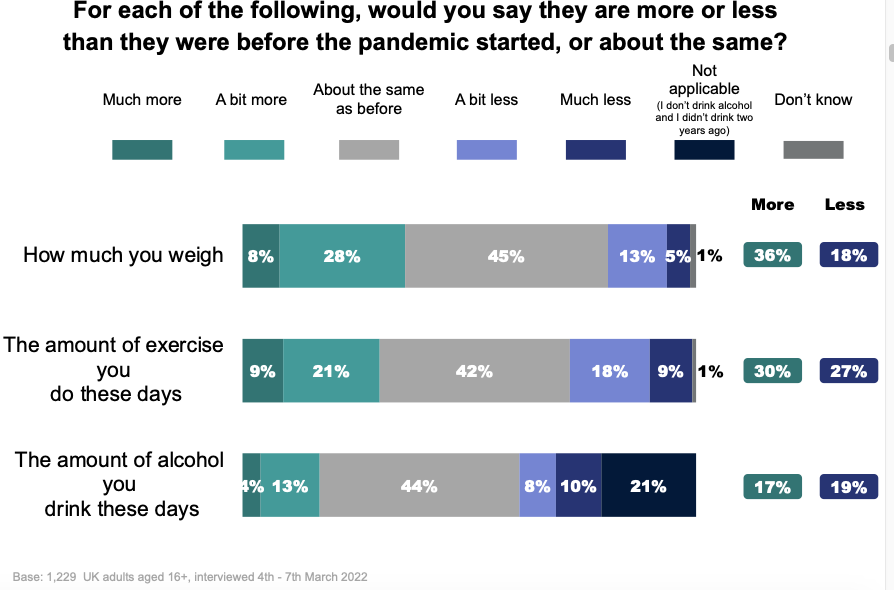
So how has the pandemic impacted on general health beyond the infections itself? Ways of measuring health can be complex, but important Western baselines clearly relate to weight, smoking, alcohol intake and levels of exercise. This survey from Kings shines some light on the impact of the pandemic.
Their finding seems to send a simple message about our divided society. In summary, about half of us haven’t been impacted very much in terms of wellbeing. For those who have, more have been negatively impacted, as described by their graphic below. While not analysed, the split will I’m sure follow the social divisions in society, with those having the resources being buffered against ill effects, and those already struggling suffering the most.
Interestingly, quality fo sleep is really important and the survey shows just the same pattern of impact of the pandemic; half OK and of the other half, twice as many doing badly. This matters as sleep quality is related to how many calories we take in the next day. Bad sleep, in other words, is one factor in putting on weight with an additional 1.2 hours a night resulting in 270Kcal less the next day, which roughly equates to 10Kg of extra fat a year.
Sleep for many can be improved, but it is clearly linked to worries and stress that are, as the survey suggests, hard wired into society. Poverty can be defined by the daily worry about money, and that is enough to impact at the end of the day when trying to sleep and all of the other distractions of the day are absent. For too many, these are hard times.
Exercise follows a similar pattern and this study show it matters for COVID19. Even when accounting for co-morbidities and other confounding factors, those exercising more did better. As the Kings study shows, this is another of those profound social issues as exercise has been driven out of much of our life. Literally.
Much of this is politics. While divisions exist in many different ways, it is at its most gross when it comes to inequality of wealth and poverty. When life is already tough, a pandemic will make it tougher. Resilience depends of resources. The political response to this is not only lacking, but as demonstrated by the recent financial statement by UK’s Chancellor Sunak, the vision is sadly more of the same.

Trickle down economics is little more than a confidence trick.
There seems to be a pervasive belief in the mythical “trickle down” effect, where conservatives believe generation of wealth automatically reduces poverty, while the evidence is crystal clear that there is a real “cascade up” of resources, increasing wealth and increasing poverty simultaneously with effects on lifestyle as seen in the survey. For economic as well as ethical reasons, this cannot go on.
A significant marker of disadvantage is eating ultra processed food which now accounts for 60% of calories eaten in the UK and is driven by financial want. If the increase in weight is persists, then expect more diabetes along with a host of obesity associated illnesses, more heath needs, and the need for more public health expenditure. We need politicians who live in the real world.
Meanwhile back in the natural world…population control for ants….
Why write about ants? Because it’s so fascinating and a distraction from the crazy human world. Hidden and interesting infections ravage the natural world around us in interesting and surprising ways. The wonderfully named Tawny Crazy and has been spreading across the US for years and causing problems. Nests of these ants co-operate rather than compete and so can spread to form super colonies that spread out for miles, out-compete native ant species and devour insects, small birds and reptiles.

Co-operation between colonies is responsible for the rise and demise of the beautifully named Tawny Crazy Ant.
Along comes a new fungi called Myrmecomorba nylanderiae (yes – why such complex names!) which specifically and very successfully predates the Crazy Ant while leaving native species alone. It seems the interconnectedness of the Crazy ant is its undoing. As soon as an individual is infected the interconnected colonies get wiped out due to rapid spread of the fungi, and its goodbye to the the Crazy ant and the ecological problems they were causing.
Slight echoes of the spread of SARS2 there with our interconnected societies causing infections somewhere to become infections everywhere. A human fungal pathogen would be harder to deal with that a viral one, as there are few therapies and no vaccines available. Let’s just leave that concept there.
Thanks for reading the blog. If you have any comments or feedback, please leave it in the box below and I’ll get back to you as soon as I can.
In the meantime, I wish you the best of health.