Summary:
- The new variant of Sars-Cov2-19 is a major setback – at Christmas in particular – and is an example of evolution taking place before our eyes.
- The effect on vaccines is expected to be minimal.
- Though not thought to cause more severe illness, it is expected to increase hospital admissions
- Lockdown and restrictions are the only way to slow (not prevent) its spread.
- PCR testing has been questioned, but remains a good test when uses in conjunction with situation and symptoms.
- The vaccine roll out has has its hiccups – did the UK cut corners?
- Anti-viral treatments remain a disappointment
- I sincerely wish you the very best Christmas you can have in the circumstances.
Introduction
Oh Dear.
Despite living in a really complex world this simple, tiny bundle of non-thinking, replicating, genetic information seems to be constantly outwitting our collective wish to live our lives in the way to which we have become accustomed.
Indeed, Sars-Cov2-19 seems to be defining what it is to live in the modern world we have created and is, right now, one step ahead of our bewildered politicians, even as it moves towards the cross-hairs of scientists.
For millions this is brought home by the loss of a festive experience so much more important than usual this year, with added frustration as Lockdown 2 and the Tier systems were introduced with the now confounded hope of giving us a break at Christmas.
 |
| Sars-Cov-2 ++ |
Last night I was listening to caller after caller on the radio in tears at the prospect of a reduced and for many, a cancelled Christmas. Then there is the loss of revenue of so many businesses who depend on a busy season, and once again, huge economic implications.
That an ever hesitant Boris Johnson has been driven to this is a statement of the gravity of the crisis facing healthcare in the face of a new and more transmissible H69 V70 variant. It may already have seeded and spread over the world and our (for once) genuine world beating capacity for genome testing is leading the way in its detection.
The timing is not good. Ask any GP when one of the busiest times of the year is for viral infections, and they will answer around and after Christmas when our unnaturally dispersed population is mixing like no other time of the year. That means that right now is probable the worst time for a potentially more transmissible strain to come along. It means that something has to be done to prevent spread – that is prevent human to human contact – even at Christmas.
So here is my round up of the news for this most unusual and for many, disappointing Christmas time as we head towards a largely uncelebrated new year, and on to all the fresh challenges of 2021.
Danger! – evolution at work
We are now witnessing evolution in action. That life defining interaction of constant genetic change with natural selection as described by Darwin in the finches pictured takes place at breakneck speed in viruses. Indeed, there have already been 4000 mutations of Sars-Cov2-19, but most of these have been very minor indeed. The virus knows nothing, it cannot think, but nonetheless is driven to replicate and whichever strain spreads best becomes dominant.
 |
| Evolution in finches |
We have been here before. A mutation involving the change in one amino acid (aspartic acid to glycine to be precise) at position 614 of the spike protein improved the effectiveness of its spike and was named D614G. This was first noticed in February and rapidly became the worlds dominant strain. Till now.
The fact that antibodies created before the earlier D614G mutation continued to be effective against it after the mutation is reassuring, but that was a more minor genetic change. If they did not, then it would suggest the new variant might require a new vaccine, and the vaccine programme not only temporarily set back, but also demonstrating the possible need for annual boosters tailored to emerging new strains, like flu. Early days as yet to make that call.
This mutation has taken place despite Sars-Cov2-19 having a clever ‘proof-reading’ gene responsible for deleting mistakes in its error (and variant-producing) prone replication cycle, typical of RNA viruses. This makes mutations less likely, though evidently, they still occur.
Milder strains too will be the ones which spread better and displace the more deadly ones which make people take to their beds and isolate, even without restrictions, so the evolutionary pressure is towards a milder pandemic. However this is not by any means certain, and this strain might just be better at spreading full stop, so keep those fingers crossed!
 |
| Image of the spike protein |
The latest mutation, variously called H69V70,VUI 2020/01 (Variant under investigation) or lineage B.1.1.7., involves 14 mutations, seven of which are in the spike protein, and was first isolated in Kent in September. Since then it has become dominant and is likely to be responsible for increased transmission and at least part of the rapidly increasing winter wave.
It is thought to have a more effective spike due to changes at its receptor binding protein, and also changes to other genes which enable it to enter the human cell more easily by invaginating itself into, and out of our cell membranes. This leads to higher viral loads, and wider spread, leading to an increase in the R0 number by about 0.4 – tipping us all up a tier or two.
I’m afraid this also results in an increase in the percentage of immune people needed to develop herd immunity and indeed threatens the whole concept in the case of Sars-Cov-19. While there is still much to be uncertain about, the significance of this is testified to by the increasing numbers of nations putting us into our own national isolation and closing their borders to us, even before Brexit. I hope this will not last long as I cannot see it being effective at keeping the new strain at bay – it just spreads too well.
Indeed it has already spread to 60 local authorities in the UK, as well as to the Netherlands, Australia and probably South Africa too, resulting in the announcement of travel restrictions which are in reality, probably too late. It is likely to have spread far and wide as Europeans and others working here have already travelled home for Christmas. When (not if) it gets to America, where control of the pandemic is so poor, its impact will be felt keenly too.
Effect on vaccines?
The vaccines contain genes for enough of the spike protein structure to suggest they will continue to be effective. We cannot go through trials of the same vaccines all over again and we will have to rely on lab experiments and epidemiological observation to learn for certain what the impact will be. I am optimistic, yet with the new strain come new uncertainties. Fingers remain crossed that the genetic changes will not lead to “escaped immunity” when vaccines lose their effectiveness.
The thought that so soon after the fanfare of the vaccine rollout, a mutation calls into uncertainty their effectiveness is irony itself. However, if we continue to make similar neutralising antibodies to the new strain it will bode well and the vaccines should continue to work – I will be keen to take my place in the vaccination queue both for my own protection, for the benefits of those around me and as the only way of heading towards any sort of herd immunity.
Watch this space!
Effect on us
The new strain seems to be rapidly replacing the old one, so clearly it is spreading more readily as shown in the graph below. Again, evolution in action. It is reasonable to assume that it is driving the increase in cases and admissions though increased movement and mixing after the end of Lockdown 2 and the increased travel at that time will also have played a part.
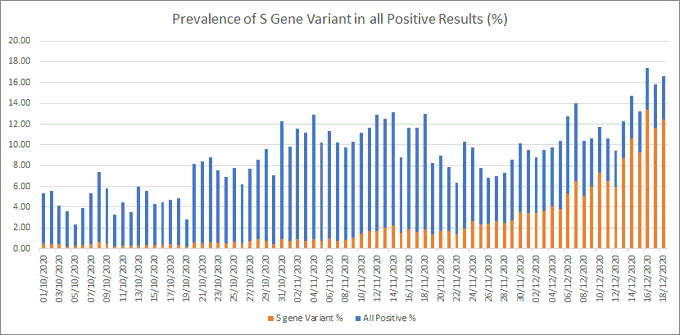 |
| Old Sars in blue, new variant in red |
There is an observation that the rate of hospitalisations has not increased, even if the absolute number has. This might mean that the new variant doesn’t cause more severe illness, but will certainly involve larger numbers of people needing hospital care in a system which is struggling in many areas due to the normal winter pressures.
Current high levels of bed occupancy means trouble in finding the relevant bed for you when admitted. I remember this well from my days as a junior doctor, when one of my essential skills was knowing exactly where the spare beds in the hospital were located when bed pressure was an issue. Since then we have shed wards and beds in the name of progress in what now seems a very false economy. Having a reasonable number of empty beds is essential, and rare.
Already this winter wave, if not taller is larger in total than the spring, means 19,000 patients in hospitals with total capacity of 170,000 beds, so 11% of all hospital beds are occupied with patients testing positive for COVID19.
 |
| Number of patients in hospital |
In many areas health services continue to cope, and the restrictions announced for Xmas are designed to keep it that way as the difference between coping and sending ambulances elsewhere is very thin.
Warnings about demand on the NHS exceeding capacity have been highlighted a week ago by the British Medical Journal and Health Services Journal, jointly (and unusually) publishing an appeal to reduce viral spread by reducing household mixing this Christmas. It is not an easy time to be in the health sector, either as a patient or staff.
 |
| Derriford Hospital Plymouth |
In my patch, Derriford Hospital was having problems before the lockdown had its effect. Three wards, (about 90 patients), were full of people with COVID19 symptoms. Since the lockdown, the number has dwindled to a very manageable 12. We have certainly been spared the worst in the South West, but the trains from London were rolling in until yesterday so we shall see what happens now. We are, co,paratively, low on ITU beds in the south west.
The impact of increased transmission due to relaxed restrictions and a strain which may be 70% more transmissible cannot be understated. While we wait for vaccination to have an impact, the NHS has to face up to a difficult and prolonged winter wave which could at its worst last till April. It is hard to imagine how hard the staff are working. Hopefully flu will be quiet this year as it is usually at its busiest in January and February.
Meanwhile…keeping one step ahead?
Lockdowns….Reducing the spread of the virus is a painful thing in our busy, dispersed, mass connected world which is almost tailored for the pandemic to take hold. We essentially have to hide from it. In the world of sceptics, there have been many questions about whether lockdowns work. To me it seems those arguments belong in the past. Despite some effect of voluntary behavioural change, Lockdown 2 seems to have answered this by the earlier significant reductions in this second wave, which have been reversed since it gave way to the Tier system and as the new variant became dominant.
All over the world there is evidence that human behaviour affects viral spread – as if evidence was needed for something as clear cut as this. Yet, after the first wave, it seemed uncertain if the lockdown was responsible for the decline, or was it due to the seasonality of the virus? Or both?
This winters experience seem to answer that question. This may be confounded by the new strain causing a new situation, but clearly the Tier system was not effective – over the next two or three weeks we shall now see once again the impact of the new more severe arrangements tailored to the more transmissible strain. The mind boggles at the hardship this is causing and going to cause in our towns and cities.
PCR Testing…..
There has also been concern in the online world that the pandemic has been exaggerated by the overuse of PCR testing, with summer reports of up to 90% of the tests being false positives.
This claim was based on a low prevalence rate in the population as opposed the higher rate in people with symptoms actually having the test done, thus exaggerating the impact of the very small number of false positives. The lower the rate in the community, the more important small numbers of false positive tests become.
The later you have the test, the less value it is, but it is reasonable to expect that those with suggestive symptoms would get a test early. Remember too that the great majority of tests are negative, and that some of these are false too. Indeed, in reality, that is more of a problem. Right now, positive tests are increasing as a percentage of total tests and so the tiny false positive rate is less important – after all, you don’t go to hospital with a case of the false positives!
Who am I to take on the New York Times, but things have certainly changed since their story and I shall post on this interesting phenomena of genuinely fake-ish news later. It’s rather technical, but not difficult to demonstrate how wildly inaccurate a good story can be and how it is magnified and amplified in the virus prone world of social media.
An appreciation of the value of the test result can be eroded by such headlines at a time when it is becoming more useful than ever to know when you are at risk of spreading the infection.
Vaccines
If you eat your meal too quickly, expect hiccups, and that is what we have had with COVID19 vaccines. I do think the speed at which a vaccine has been developed is something to celebrate – a real achievement brought about by need and necessity.
That there has been allergic reactions in two people given their first dose of the Pfizer vaccine already know to be prone to anaphylaxis is no surprise. The individuals will not have the booster, but will get significant protection (82%) from the first dose on its own and the roll out proceeds while the Oxford/Astra Zeneca vaccine tries to catch up from behind.

It was hardly unexpected that the UK would tiresomely repeat its “world beating” mantra by vaccinating the first non-trial person. Might these headlines have been generated at the cost of this early cock-up? People with anaphylaxis were not included in the trials and not to exclude them in the vaccine roll out, (now done), is a major cock-up.
Worse still to talk in the media of excluding people with ‘severe allergy‘, when it is only those with a history of anaphylaxis who need to be excluded. As a consequence, people vaccinated will now have to hang around for 15 minutes after vaccination, seriously complicating the logistics.
Might this have been predicted by looking more carefully at the raw data instead of rushing towards a finishing line of their own creation? American and EU regulators certainly think the UK have cut corners. Trust is very important in vaccination trials and I wish our government would be less hasty in grabbing headlines.
The hint that this was a Brexit bonus was even more dishonest as such decisions could always be taken by member states. Perhaps this is our Unique Selling Point – cutting regulatory corners – something to watch for a we head to a no-deal or crap-divorce from our neighbours.
With the Pfizer vaccine the brainchild of Turkish immigrants to Germany working in collaboration with American Pharma, to deliver a vaccine manufactured in Belgium, the only way to spin this to a world beater for the UK was to give approval before waiting for the raw data and relying on company information only. The FDA and EU procedures have been more thorough and asked more questions when compared to the British rubber stamp.
Such consideration will fade as the global rollout gathers pace. Widespread coverage of those at risk of the illness or of spreaging it will be fantastic and have a real impact on our new world. There are lots of issues to face, economic, social and political, but as I have said, I will take my place in the queue and have the vaccine with enthusiasm.
Treatments
Despite 2,800 trials on new drug treatment for COVID, it is a big disappointment that none have emerged as useful other than dexamethasone. According to the WHO’s living guidelines, built on results from these trials, remdesivir, lopinavir, hydroxychloroquine and interferon have had no significant benefit for patients.
Despite this, treatment with remdesivir has become pretty standard treatment in the US, despite failing in trials and now will be hard to withdraw, despite its cost and lack of effectiveness. Dexamethasone helps if given at the right time to the right person, and vitamin D should be used far more widely in view of positive results from Spain and increased understanding of its roles in our immune system.
It remains unloved by the scientists from NICE, but a good quality trial showed definite benefit in reducing admissions to ITU in hospitalised patients and while further results are awaited, I will certainly continue to take mine.
Other than that, anti-viral treatments have been a big disappointment. Claims that hydroxychloroquine is effective have been debunked both in terms of progress of hospital admissions and failure to prevent infection in those in contact with cases. Some continue to claim they work in a poorly defined out patient setting.
The internet is full of, such claims, most recently in a senate hearing. These are easily de-bunked. That is why randomised controlled trials are so important when it comes to treatment with drugs where wanted have to be balanced against unwanted side effects.
The WHO’s central role here is a model for the future in terms of sorting out the small amount of medicinal wheat from the piles of chemical chaff. The Oxford based RECOVERY trial has a trailblazer for defining what does less harm than good.
Happy Christmas…

Another wise and compassionate epistle, Colin…many thanks xx
Thanks so much x
Beautifully written, informative and balanced Colin. Sending much love to all of the Bannons.