Summary
- Omicron is a less severe infection for most people but will continue to cause problems.
- COVID19 will continue to have an impact on critical aspects of society, particularly healthcare.
- Excess deaths are very unlikely to have anything to do with vaccination.
- Millions remain vulnerable to infection and will benefit from autumn boosters.
- The evidence is stacking up that the pandemic originated from a spillover from the natural world.
So goodbye to the sixth COVID wave, or it the seventh? I forget. Those times when infections are low seem to occur briefly in between waves caused by the latest update from the ever changing virus. Despite early hopes that the virus might be more stable, in reality it mutates pretty quickly and its rapid evolution to variants with faster transmission is evident before our eyes. COVID19 has shifted from the news, understandably so, but it has not gone away.

The unprecedented increases in energy prices, the summer heatwaves with and the lack of any progress at all towards a cease fire in Ukraine all have big implications for the future, occupy the mind and put COVID in the shade. We live in a world of ongoing crises.
Having an absentee Government in the UK at such a critical time doesn’t help, though in the case of Boris Johnson’s, perhaps a rudderless ship is a better than being steered onto the rocks? I know of no one eagerly anticipating Truss’s leadership the country and much of her Victorian thinking there are surely more crises around the corner. As if all this isn’t enough, COVID remains important to understand with decisions coming up regarding boosters and behaviour this winter.

Personally, I seem to be one of the very few people I know who still have not had the infection, at least as far as I know. This seems some sort of achievement considering plenty of people close to me have had COVID recently, some of whom only tested positive after multiple tests. For some, it was a nasty infection though thankfully all I know have recovered well. This begs some questions: What is the latest variant doing? What about vaccines and boosting? Time for an update……
Omicron – better news.
Omicron is certainly milder than its ancestors with symptoms lasting on average for 7 rather than 9 days and down to 4.4 days for those vaccinated and boosted. Loss of smell is reported by 17% of those with Omicron against 53% with Delta. There is a 25% less chance of hospital admission and a 2.5 times better chance of being recovered in a week. Hospital admission rates are further reduced when incidental infections are excluded, important with a milder illness. Taking this into account, vaccine effectiveness (risk reduction for admission) is 75% even once the immediate infection preventing effect of the booster had faded.
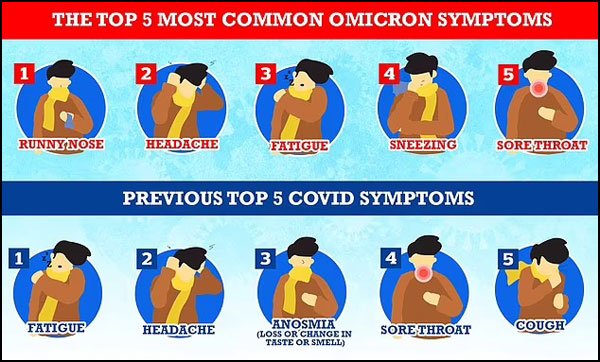
COVID19’s changing symptoms.
Gloomily there have been headlines about catching the virus on many occasions, including soon after the last, suggesting in particular that natural immunity offers little benefit after an Omicron infection. For many, one infection is bad enough; multiple infections a year would be hideous. But it this just more sensationalist nonsense? Mainly yes.
This study of people who have the Ba4 or 5 infections and their previous exposure in Qatar shows pretty clearly that infection continues to deliver at least some immunity. In essence:
“The researchers found that infection with a pre-Omicron variant prevented reinfection with BA.4 or BA.5 with an effectiveness of 28.3%, and prevented symptomatic reinfection with either subvariant with an effectiveness of 15.1%. Prior infection with Omicron granted stronger protection: it was 79.7% effective at preventing BA.4 and BA.5 reinfection and 76.1% effective at preventing symptomatic reinfection.”
So you can get re-infected with Omicron, but the chances are against it, at least for the two months looked at. Also the study is about any infection, not illness. I have heard more realistically that on average we might all have an infection every three years, but with reducing risk (fingers crossed) of it causing problems in the short or long term.
The forever pandemic?

So will this just go on for ever? In a word, no. Not forever, just for a generation. Kids repeatedly exposed to the virus or vaccine build up immunity which has the potential for them not to be too troubled by infections as adults, one of the few ways youngsters are lucky in this day and age.
For the rest of us, COVID19 will add to all the other threats to our health and particularly that significant chunk of the population who are vulnerable and on whom, medical and social care services are concentrated.
In the US, this means a big chunk of the astonishing 94% of people whose metabolic health is not ideal; this includes those with obesity, hypertension, poor blood glucose or cholesterol, or established heart disease. Thats a huge number of people whose vulnerability to COVID is increased and why the pandemic has brought to sharp focus, many of the other problems of human health, like the Western diet.
It will therefore continue to shorten life expectancy and add one more way to depart this mortal coil for the aged and vulnerable. America did particularly badly at protecting its population against the pandemic though the 2 year drop in life expectancy was not only due to infection but also due to the lack of resilience due to poor welfare services. Again, too much wealth and too much poverty.
COVID 19 will also stretch an overstretched health services and make the hospital experience that more difficult for all, from the trivial inconvenience of having to wear masks to more life threatening waits to be seen in A+E, delays in non urgent care and ever lengthening waiting lists. In summary, we will have to get used to worse health care unless there is a big change in the way we see the link between the economy and health.
As ever, prevention is better than cure, so whats happening in the world of vaccination?
Vaccines do not cause excess deaths
There have been 10% more deaths than expected in the UK and elsewhere this summer. Most of the deaths have been due to heart attacks, stroke or the complications of diabetes and are likely to be due to a number of factors, yet to be accurately determined. This of course leaves a gap into which the ever opportunistic antivaccine community jump, claiming the association with the booster campaign explains it away and thus highlights the crimes of the medical and scientific community.

As ever anti-vaccination folk love a scare story – the picture shows old protests against vaccinia inoculation against smallpox – but the reality is far more nuanced.
One far more likely scenario is exactly the opposite. This Korean study looked back at the records of a quarter of a million people diagnosed with COVID in South Korea. They found the risk of admission with heart attacks or strokes were reduced by 60% in the three months following infection in the vaccinated compared to the unvaccinated. That is despite the unvaccinated having less pre-existing medical problems than the vaccinated and strongly suggests that vaccination protects against excess deaths sen after COVID19 infection.
It may not be the end of the story. The summer heatwave, financial stresses, the general feeling of ongoing crisis, saving evaporating into the oil producers pockets, a struggling health sector and long waits in ambulances are among the many other factors at play. That skeptics put this down to the boosters enhances my feeling that growing anti-medicine and anti science is a real threat to the health of those vulnerable enough to be taken in by it all.
The ‘old’ vaccines
An update of a study of the benefit offered by vaccination and boosting shows that protection against hospitalisation or visits to Emergency departments was an impressive 83%/76% up to 3m after the booster, and still 79%/74% thereafter, showing little waning at all. This is better news after earlier studies showed more rapid waning, but were skewed by the immunocompromised being heavily represented as they were the priority for the shots.

This UK based study shows that previous infection with Omicron prevented re-infection in 45% in the unvaccinated; previous vaccination prevented 81% of hospital admissions with little waning after 3 months. Interestingly, infection after vaccination only added an extra 4% protection. In other words, vaccines work!
Reassuringly, it went on to conclude: “mRNA booster vaccination was still found to be highly protective against hospitalisation and death in omicron breakthrough cases”
There are also encouraging results from Denmark where reduction in vaccine protection against hospitalisation was due to more incidental infections in the hospitalised from a milder variant which also skews the figures. When respiratory illness from COVID was used, effectiveness of the vaccine against hospitalisation is holding up well.
The conclusion seems to be that vaccines effectiveness at preventing infection wanes pretty quickly, but effectiveness against severe disease hold up far better. More information will come along after the summer and be published later in the Autumn, but there are solid reasons for optimism that the vaccines have done well, but that protection against any infection was always going to wane, as it does with many other infectious illnesses like flu.
‘New’ vaccines
Given all that, there has been a race to produce more up to date vaccines with the big players all developing ‘bivalent’ vaccines to include the Omicron strain. Moderna have just sold 13 million doses of a bivalent vaccine (Wuhan and Omicron B.1) to the UK which is the first country to buy them in readiness for a booster campaign later in the year.
Dr Paul Offit is one of my go-to experts on vaccines. He was the inventor of the rotavirus vaccine and has thus saved the lives of countless children. Yet, he was the dissenting voice on the the FDA advisory panel which recommended the widespread use of boosters. His reasoning is that the original vaccine is working well enough at preventing serious disease so boosting is sensible for those whose immune systems are impaired, which admittedly, is quite a large number of Americans. This is further defined by those demographic groups ending up with hospital admissions rather than boosting healthier people whose protection from the initial vaccine seems to be holding up.
This precedes the development of a COVID wide vaccine. Nanoparticle bases vaccines with multiple spike versions on them, vaccines with ‘chimeric’ proteins which resemble different strains or viruses are potentially in the pipeline and the hunt for more stable parts of the virus to target goes on. Such vaccines would cover more, perhaps all variants, but not it seems this will not be ready for this winter. I wonder if the political will is there to adequately fund the programmes? Politicians have very short memories, shifting priorities and it seems, a declining awareness of science.
Vaccinating children
The US have decided to recommend vaccinating the under 5’s, but it is uncertain if other nations will follow. The illness in under 5’s is usually mild, but in the first year of the pandemic, 25 children under 12 in the UK died from COVID19, 19 whom had other illnesses, and this likely to be less with new variants. There are far more deaths children in low and middle income countries, so vaccinating the young there might be more reasonable, but in the UK we are not set to recommend vaccination for the under 5’s any time soon.
Old enemies
What might be more important is to concentrate of vaccination programmes against the deadly diseases which might be re-emerging. Polio has made an appearance in the US, Israel and London with two cases of paralysis reported after detection of the virus in sewage. Sadly, the first case of Diphtheria has been reported in Australia with the affected unvaccinated toddler in ITU. Polio and Diphtheria are horrible diseases and any re-emergence makes increasing rates of vaccination against them a priority. This means that focusing resources on these illness and like adults considering boosters, COVID vaccine for the young could be focused on those with vulnerabilities.
So who needs boosting?
Given that vaccine protection against mild infection is always going to be transient, and that protection against severe illness is holding up, who is it that needs further boosting? The answer is both complex and simple. Anyone for whom an infection will be a serious threat – that is those with medical problems, the aged whose immune systems are winding down, as well as those who are obese, smokers, and the physically unfit could potentially benefit. Then of course, are those who are in regular contact with the unwell, so the numbers who might benefit from boosters is significant. After more than two years of infections and vaccinations the situation is different from the initial drive for mass vaccination.

For younger people and the healthy, why continue to offer vaccination to avoid an illness which they can generally manage? Take up seems to be falling, particularly in the US where mixed messages have caused confusion and misinformation is rife.
Of course, it’s not all about hospitalisations or death. A big issue is long COVID, defined as symptoms longer than 4 weeks. Again, the risks are reduced with Omicron to a still significant 4.5% from 10.8% with Delta. That is a large number of people, (1.7 million as of March 22) but the risks are lower. There are also the economic problems caused by large numbers of people off work, a real issue for those in the healthcare sector, anyone who needs their help, as well as the range of public services we all depend on for getting by day by day.
When a middle aged GP, I agreed with my partners to have annual flu shots not because I was worried about getting flu, but because I wanted to avoid time off in a busy surgery in the winter. Im sure there will be some who want to get boosters for similar reasons.
Then there is treatment….
Paxlovid
This remains the mainstay for vulnerable people with symptomatic illness. It may well work better for them than the more disappointing trial results when fitter people are included. When confined to those at most risk, the benefits remain impressive. As usual, this excellent blog is my go to for up to date news about treatments and vaccines and all things viral.
Back to the beginning
We are brought back to the beginning of the pandemic, now seeming such a long time ago, and the origin of its ongoing global impacts by two new studies which provide further evidence that the pandemic originated in a spillover from the natural world. The first, shows that Coronavirus susceptible animals were being sold in Wuhan market, that the early cases were geographically centred in the market and that environmental samples tied in with the location of market vendors selling live animals.

Like the Monty Python parrot, the “lab-leak” theory might be dead, but will be forever claimed to be alive and well by believers.
Another study of the genetics of the virus at the time of its arrival shows that two strains, A and B were in circulation in early November 2019 and points, as with so many other pathogens, to its origin being from multiple spillover events from the wild.
Not absolute ‘proof’ it might be said, but they add to the many other studies pointing to our complex and global abuse of the environment being the root cause of the pandemic.
This won’t put to bed wishful thinking that it was a simple laboratory accident, or the notions that its all been arranged to usher in a new world order, (as if the old one is a rip roaring success!) but at least it might help defuse one of the glowing fuses between China and the USA.
Thanks for reading the blog and well done if you have got this far. Please do leave any questions or comments in the box below and I’ll get in touch as soon as I can.
Colin, thanks for the article. I am still not convinced of the Wet market origin for Covid. The evidence shows that it was a focus for infection, and a very effective one. And that is all that the Worobey paper you reference shows is that. But the fact that a lot of cases originated there, if applied to bananas in the UK would lead to Welwyn Garden City as the origin of the banana as that is where Tesco has its HQ and has garden in its name, which confirms it. But that very wet market, was a few miles from the Wuhan institute of Virology but a mere 300 metres from the Wuhan CDC laboratories which at this time had also acquired bats – from the Wuhan Institute. Worobey also makes great importance as to the date of the earliest case being from the wet market, but we know of an UK case (who was in China at the time) was 3 weeks before his case zero. But that case may well have been to the Wet Market! So we know the virus pre-dates Worobey’s data by at least a month. As for the concentration of cases around the market, well that is where the authorities were looking for cases- so they were bound to find cases there so that puts another bias onto the data.
The second paper confirms that the virus pre-dates Worobey’s data. It also states that there were 2 strains very early in the epidemic. So it comes to the conclusion that -all of the circumstantial evidence so far points to more than one zoonotic event occurring in Huanan market in Wuhan, China, likely during November–December 2019.-
So we have been living with Wet markets all over the far east for hundreds of years. The last cross over of a coronavirus to man is believed to have happened in 1889 (the Russian Flu epidemic), which puts such events in the order of a century, though as humans we seem only to be susceptible to some half a dozen coronavirus species which would suggest that my once in a century crossover estimate is too frequent.
So, we are to believe that “of all the wet fish markets in all the towns in all the world, she walks into mine” twice in a month
Thanks Owen, very interesting. I guess the Tesco analogy breaks down if we consider that one banana might have been brought there from its source and then the WGC site manufactured the rest. We have MERS and what can reasonably be called SARS1 as crossover events and there are plenty of others. Plausibility has to play a part and also acceptance that with the secrecy of NIH and the growing enmity with China it will be impossible to prove something didn’t happen. Further, in this age of climate and ecosystem breakdown, the important message could not be more clear, we have messed with the nature we depend on beyond its tolerance and when that happens, we are in big trouble. I still feel for the bats, flying further and further to get less food, and their own immune systems strained by the task, enabling infections and viral evolution to take place. I’m not a big fan of GOF experiments, but virology institutes have to do more to take the public with them in explaining what they are doing, why and what benefits there might be. Thanks again.
Hi Colin. Thank you for another excellent article – love the addition of the cartoons!
Thanks Tricia. I hope all is well with you