Introduction
Despite the global unmet need for vaccination the current situation means that a booster campaign is under way in northern nations. Lets have a look at why this is necessary and what the boosters do.
The current situation
Infections here are grumbling along, though it is clear that most cases are in schoolchildren and youngsters who are not longer subject to lockdown or restrictions; this means the balance has been shifted in favour of easy viral spread among the largely unvaccinated. To some extent, it had to be this way; kids could no longer miss out on school and vital socialising which school offers.
Yet an over relaxed attitude to viral spread has been a political decision which has contributed to hospital admissions running at about 1000 a day, and deaths at about 200 a day, about four times the levels in Italy. There masking and social distancing is combined with a Green Pass and seems to be making a real difference. Here, the Government feel the health impact is a price worth paying for a more liberal approach.

Put it back on Boris!
In the last week there has been a drop in cases in terms of positive tests, though this is far from certain to continue. Some of the drop in infections might well be due to less testing during half term. The ZOE symptom tracker suggests upwards of 90,000 new infections a day though also perhaps having reached a peak. This is about double the number of positive test on the Dept of Health website. The ONS infection tracker also shows about 1 person in 50 currently infected.

So this is disappointing. While the vaccines remain very good at preventing hospital admission and death, even effectiveness of 90% means that there will be a trickle of infections, including in many who have been vaccinated. This particularly applies to us elders, and our creaking immune systems – immunosenescence. In particular our ‘spare’ white cells that can become new B and T memory cells capable of remembering and infection for next time have largely been used up. Plus of course all those other vulnerabilities which come with age.
It may well also demonstrate how effective lockdowns and restrictions are. Conversely, heading to the winter with a government determined to kick difficult decisions into the long grass, few significant restrictions means that protection from a booster will be welcome for those who need it most.
Immunity
I have to start by saying our immune systems are pretty impressive. In experiments on mild cold coronaviruses, infected volunteers had protection for a year, and re-infections were mild. With flu it seems that protection against infection after the flu jab drops by about 7% a month. The flu pandemic of 1919 showed how previous infection can be protective for some time – younger people least exposed to previous infection fared the worst.
After what we can now reasonably call SARS1, protection in terms of T and B memory cells persists to this day. This study showed that Natural Killer cells persist and offer protection for up to 9 months and likely beyond after moderate SARS2 infection. The average age was 54 with follow up to 250 days. For most of us, that is encouraging
Yet with SARS 2 Delta variant, much uncertainty exists and its increased transmissibility to vulnerable groups makes it different. I would expect some waning in antibody levels, but in the populations most at risk, T and B cell precursors may not be available to offer longer term protection. This is important for anyone who is older, has vulnerability of any kind, or is caring for or in contact with those at risk – that includes an awful lot of the population.
Coupled with that is that any waning of vaccine effectiveness, or immunity from infection will be happening in those groups vaccinated earliest and most at risk. There are arguments against this; antibody levels can reasonable drop after infection or vaccination, if not our blood would be clogged up with the vast array of antibodies after a lifetime of exposure to foreign proteins. They increase once again after exposure to remembered foes.
Add to that the significant numbers of people with diabetes, pre diabetes, high blood pressure, and a host of other ‘western’ illnesses and you have a recipe for overload of the NHS with implications for us all.
Why have a booster?
Welcome November frosts ( I love ‘normal’ weather) hints that we will soon be in the winter when the virus is more likely to spread. Viruses like the lower humidity, the indoors, crowds, and of course the festive season is always a gigantic mass spreading event in itself. The more viruses around now, the more infections we will see later as we become winter bound and the virus spreads.

It’s that time of year again……
That being the case, and given the excess number of vaccines bought by the UK and USA, it seems more reasonable to offer boosters to those most at risk of breakthrough infections as the winter approaches.
Ethical concerns regarding basic vaccination in the poorer nations persist – COVAX has not been a resounding success. But here too we have our problems with a creaking underfunded, demoralised health sector. If there are significant problems for the NHS this winter, we may discover what it is like to be a second world country. Adding to this is the staffing crisis. The latest two medical acquaintances I bumped into are both taking early retirement. That reflects a worrying trend and means that we will be well advised to err on the side of caution.
What effect does a booster dose have?
Earlier in the year this study showed that antibody levels after a third AZO vaccine were twice as high as with two and this reflects the immune systems ability to remember the spike protein and produce a good response when challenged.

In other words, the vaccinations seems to be doing exactly what they are meant to and a booster works well, promoting antibody production and the development of immune memory.
Israel was the first to vaccinate its population and took an early lead which was overtaken by others as time went by. As a consequence, they started a booster campaign first and are first to post some impressive early results – an 11 fold reduction in infections and 19 fold reduction in serious illness in the 12 days after the booster. So it certainly seems to work in the very short term and suggests that if maintained, benefits will last through the winter and have a big impact on stresses in the winter, both for millions of vulnerable people.
A unpublished study from Pfizer showed that in the 5,000 people who received the booster dose, 5 of them developed Covid-19 illness. In the 5,000 people who didn’t get the booster (but were double vaccinated) there were 109 cases of Covid-19. This was over 5 months in those vaccinated 11 months earlier. In other words, the booster was 95% effective at preventing infection.
The hope remains that as community immunity develops further and the booster campaign protects the vulnerable we can get through the winter and look forward to an optimistic spring and potentially the end of the pandemic.
Why not a Delta specific booster?
In short because the manufacturers feel that the current vaccines are working well enough for the majority of people and that a booster with the same vaccine will works well enough against the Delta variant also. They have performed small trials – trials of trials – on small number of people with a Delta specific vaccine, but the bigger trials needed to demonstrate safety are being held back for a more deadly variant.
It is possible to develop vaccines which code for proteins of a number of different variants, rather like we do with quadrivalent flu vaccines, but that time seems yet to have arrived, and indeed may never arrive. For a booster of current vaccines give adequate protection.
Who will get the choice – Immunosenescence

There are even textbooks on it….
For many, immunity is holding up well and boosters are not needed, and may well never be. The JCVI recommend the following groups will benefit:
- those living in residential care homes for older adults
- all adults aged 50 years or over
- frontline health and social care workers
- all those aged 16 to 49 years with underlying health conditions that put them at higher risk of severe COVID-19 (as set out in the green book), and adult carers
- adult household contacts (aged 16 or over) of immunosuppressed individuals.
For people with MS
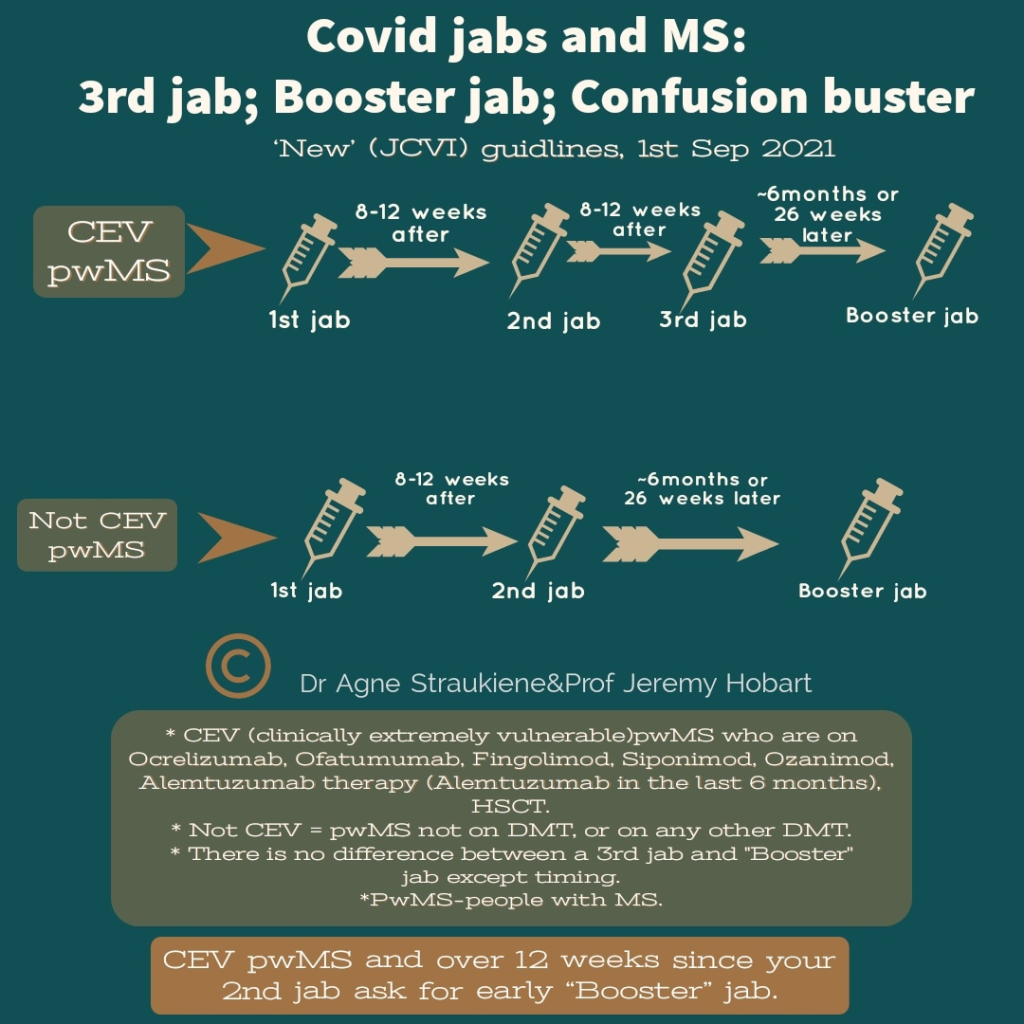
Thus graphic produced by our local consultants sums up the situation for people with MS, first those clinically extremely vulnerable (CEV) and then those not.
Which booster to have?
In the UK, the vast majority of us have had the AZO vaccine which the US didn’t want. Despite having advantages in terms of cost and ease of transport and storage, it is not quite as effective as the mRNA vaccines though its immunity may last longer.
The official advice for the booster is to have the BioNTec vaccine which the COV-Boost trial, according to the JCVI, shows that the vaccine is well tolerated as a booster and shows a better immune response. Alternatives are a half dose of Moderna, and for anyone who had problems with the mRNA vaccines, AZO is available.
So it’s mRNA vaccines, starting with those who were vaccinated first with a 6 month delay, so my own booster will come along late in November. As early as April 21 the UK government bought 60 million more Pfizer vaccines in anticipation for the need for a booster campaign to add to our vast stockpile of vaccines.
Make vaccines more effective with Vitamin D.
With the winter on us, our Vitamin D levels are dropping and the indoor life becoming the norm for billions of people, in particular, those people vulnerable to the infection. It makes sense to maintain levels of Vitamin D which is essential for immune health, and lacking due to a diet lacking in fresh oily fish and indoor life.

The winter sun, though beautiful, doesn’t lead to much Vitamin D synthesis in the skin, so supplements are sensible.
Without going into a long, dull analysis of the data on this, it makes perfect sense to correct a deficiency for which the rationale is so powerful. The CORONAVIT study will, I hope shed some more light on this, but has yet to publish, Till then, all the advice about prehabilitation I described a year ago remain true and it makes perfect sense to get as fit as possible, with VIt D supplements being one component of this.
Will boosters become the norm?
Perhaps not. Some vaccines, like tetanus and Hepatitis B are given in three doses and give long lasting immunity. As I have said before, the virus may mutate into something more transmissible and milder leading to dominance of variants which will become, as in the past, a flu like illness or a cold.
Sars-Cov-2 is not like flu, whose surface proteins change substantially from one year to the next, giving new strains that evade previous immunity. The mutations leading to SARS2 variants are more subtle and it can reasonably be dealt with by prior immunity.
With over 90% of us having some protection against SARS2, the disease is already becoming milder. With infections now spreading rapidly among the young with their nimble immune systems, the hope is community immunity can only improve with time.
The virus will find less and less vulnerable people and fizzle out, leading to infections with highly transmissible and milder variants and then become a mild seasonal illness which we will all be able to cope with.
So then we will be able to look back on the pandemic. It has highlighted the vulnerability of our species to the forces of nature, our weak political systems, corrupt leadership, and the mind damaging potential of misinformation and lies, but also the potential of science to get things done and to take the population with them. As the pandemic fades COP21 hints at the possibilities for much bigger changes we now need to see happen.
The new normal cannot be the old abnormal.
Thanks
If you have got this far, then thanks and well done. If there is anything you would like to say, state or comment on then please do so in the box below and in the meantime, I wish you the best of health.
Hi Colin, what is the best course of action for those that have been double vaccinated but then subsequently had covid? Should the booster be 6 months after the second vaccine, or 6 months after the covid infection (which is 2 months later). Been meaning to ask!
Hi B. Sorry about the delay. Recommendations vary, but it seems to me that there is a good immune response to infection, particularly when there has been lots of symptoms. If I was in this situation, I would leave any booster for 6 months after infection.
Many thanks, Colin, for setting out where we are and how best to look after ourselves.
Take care,
Jackie xx
Hi Colin, as always a very well written piece. I was wondering what your thoughts are about pwMS having their covid booster jab at the same time as the flu jab (in different arms)? Thank you.
Hi Jayne. Yes the official advice is that this is OK to do, just depends how you want to play it – get it over at once or separate any side effects. Personal choice really – would make it easier for the staff to have both at once…
yes indeed, would make it easier for staffing. Thanks Colin.
Thanks for your clarity of the explanation
Your very welcome