Summary:
- The Delta wave has seen increases in COVID cases here and around the world.
- The variant is more transmissible and questions have been asked about well the vaccine is working
- A look at the evidence showing the vaccines continue to be effective.
- Why vaccines continue to reduce transmission and why claims that they don’t are way off the mark.
- A look at the difficulties of balancing safety against the need to get out and about and have fun.
Introduction
Having seen off the winter wave many were looking forward to a virus free summer with lots of fun and frolics. Then along came the Delta variant with its increased ability to jump from person to person and make the illness worse. Around the world this was followed by climbing cases, more people admitted to hospital and sadly more deaths. All very disappointing, if not entirely unexpected.
Accompanying all this are concerns that vaccines are failing, in particular in their ability to prevent spread – so let’s have a look at whats going on, and of course, when it comes to over-reaction and misinformation, we have to start in the USA:
Uneducated States of America
After Biden’s initial success, the pandemic flared up due to the Delta variant, with reduced mask wearing and relaxed social distancing helping it along, particularly in states with low vaccination rates.
In the US, though patchy, there are low rates of vaccination in populations susceptible to well funded anti vaccine publicity – 22% of Americans now define themselves as anti vaccine. This may not be surprising as nearly 40% of the population in the USA believe that we humans have always existed exactly as we are, a concept demolished by the most flippant glimpse at glaringly obvious evidence for evolution.
Carl Sagan, the brightest of American science philosophers rightly railed against the poor understanding of basic science in the US. In 1997 in his book “The Demon Haunted World” he lamented that 63% of Americans were unaware that the last dinosaur died before humans arose and that half of Americans don’t realise that the earth goes around the sun and does so once a year.

As Leonard Cohen once sang, the USA is the cradle of the best and the worst – especially when it comes to feelings about vaccination.
Things may have improved since; I wonder, but it is against this semi-illiterate background that COVID19 pandemic arrived with all its nuances.
Initial confidence in the vaccines ability to prevent spread was shaken by a largely Delta variant outbreak in Provincetown in the US. There, 74% of the 469 cases were fully vaccinated; 79% had symptoms, five were admitted to hospital, four of whom were vaccinated; thankfully no one died. The Ct values (a way of measuring viral load) of the PCR test showed similar values in vaccinated and unvaccinated folk, and led to the US CDC retracting their overblown claim that vaccinees don’t spread infection and encouraged even more noise from those who like to think they never do. Confusion reigned and much of this was made by the anti vaccine movement!

The Provincetown outbreak took at a large festival where the CDC reported: “persons with COVID-19 reported attending densely packed indoor and outdoor events at venues that included bars, restaurants, guest houses, and rental homes.”
Perhaps after all, some care was needed when attending crowded indoor events where the booze was flowing and guards were down.
Now with Americans being urged to dust off their masks and reintroduce some degree of social distancing, the claims that vaccination doesn’t prevent transmission is being embedded in the minds and thinking of those who like to see it that way, and more importantly for some the perceived lack of protection for others encourages hesitancy. So what is the reality?
Transmission – the reality
In a world of uncertainty, one thing is certain:
VACCINATED PEOPLE DO NOT SPREAD THE VIRUS NEARLY AS MUCH AS THE UNVACCINATED.
So how can I say this with such emboldened confidence?
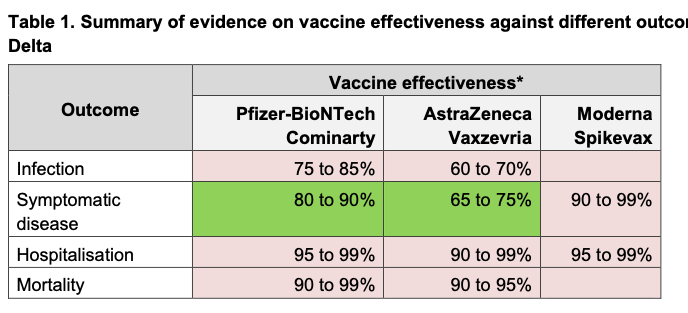
For one thing, vaccination continues to be an effective way of preventing infection. Even the worst estimates suggest protection against the Delta variant of 60% in the UK from the AZO vaccine, and if you haven’t got the infection, you cant give it to anyone else.
Thus your vaccination reduces your chance of transmitting the infection by at least 60%. Well done! The latest figures are shown here:
This is borne out by data from New York where 95% of people admitted with COVID19 are unvaccinated.
So what happens to your contacts if you are vaccinated and get infected?
This study of over 300,000 people from earlier in the year showed that even after a single vaccination you are 40-50% less likely to transmit your infection to other household members. Although almost impossible to study, it seems reasonable to suggest that reductions in spread to those with whom you have less contact would be even greater.
Then along came Delta followed with those headlines claiming that vaccinated people can spread the virus, correct of course, but also claiming that they are as infectious as unvaccinated – wrong.
Remember the Provincetown CT values? The Ct (cycle threshold) value is that number of repeat amplifications needed to detect viral RNA on a PCR test. The lower the number, the more virus there is around, the bigger the number the less there is.
It seems that the viral load from anyone coming across the Delta virus will be higher that the Alpha. It is more transmissible. In the Provincetown outbreak, Ct Levels were equally high in vaccinated and unvaccinated and from that spread the notion that vaccination has no effect on spread – yet there is more to this than meets the eye.
Essentially, those with immunity have antibodies on the surface of the mucosa lining the nose and throat and antibodies in the blood. These, together with pre primed T and B cells, despite the initial viral blast, will immediately start neutralising the virus way quicker than those with no immunity at all.
Research shows that despite similar initial CT values among vaccinated and unvaccinated, the vaccinated start clearing the virus more quickly, taking 5.5 days to eliminate the virus as compared to 7.5 for the unvaccinated, equating to a 27% reduction in risk.
Another incredibly thorough study of the Delta variant in China showed vaccinated people had approximately 3-fold decrease in the quantity of viral RNA copies, which again means less transmission. That was with the less effective Sinovac jab. They conclude: “vaccines appeared to be effective in reducing transmission of Delta infections and high vaccination coverage should be pursued to reduce the burden of COVID-19 pandemic”
In Summary:
Vaccinees are at least 60% less likely to get infected and those who have breakthrough infections have a 27% shorter duration of carriage, and a far less total viral burden. So those vaccinated are far less likely to transmit the infection, probably in the order of 80% in total.
So well done again to those who have been vaccinated and for those who have had an infection and got away with it without too much harm being done.
How can we reduce risk further?
Over here in the UK we have decided to allow pretty much normal mixing, big events, and minimal prevention. This has increased spread and the number of infections, though with far less resultant hospital cases and deaths – a huge real life demonstration of the benefits of immunity, mainly due to vaccination and also wild infection.
Central advice to continue with mask wearing and social distancing would have saved lives, but Bo-Jo decided they were not worth the inconvenience, though did later suggest that people should wear masks when in crowded gatherings, rather like this:

Bo-Jo and chums shortly after advising us to wear masks in crowded places.
Controversy has raged over here when the government announced that only double vaccinated people would be able to attend nightclubs. This advice was junked after howls of protest from the nightlife industry who rightly felt that policing such a directive would be impossible and potentially ruinous as their clientele come mainly from the less vaccinated young.
A compromise seems reasonable. The NHS pass is often used for this purpose and is available to anyone vaccinated, and to anyone with a positive PCR in the last 6 months. Personally I think the latter could be extended to a year, and perhaps indefinitely. Add to that a negative PCR or Lateral flow test and you have the best balance of reducing risk while maintaining vital social interaction for everyone. Minimising, though not eliminating risk.

The NHS Pass – For anyone with proven immunity.
Profitable flow tests.
The rapid LFTs continue to be available freely yet are not without their problems. I have posted before on their huge costs and how the cash zooming into some very dubious pockets could be better used. It is actually beyond my investigative effort or skills to find out the cost per test, though some have estimated about £8 per go.

By 26 May, of the 691 million tests distributed in England, only 96 million (14%) had been registered as used on Test and Trace, the rest having been used without registering the result or remain on shelves in cupboards. Either that or the results are overwhelmingly negative, as reported in the Liverpool pilot.
This spending roughly equates to the £20 ‘uplift’ on Universal Benefit which costs about £6bn a year which is likely to have far more positive public health benefits than current spending on lateral flow tests. (Scrapping the £20 for Universal Benefit is in effect a 12% pay-cut those those in most need.)
Of course, it is not either or, but the scale of spending on LFT’s is enormous for benefits which when examined, don’t make a big impact on public health.
Another problem is their high false negative rate. This is in part caused by understandably poor technique – it is not easy to correctly swab very sensitive areas of the nose and throat, and there will be a certain bias in those who are desperate to get through the doors of a nightclub or into a festival or event. 40% of people with an infection will be falsely reassured, though 60% rightly so – its playing the odds.
More usefully, a positive test is pretty good at getting it right if you are infected though the chances of this being helpful depends of how common COVID19 is in your area. See this interactive guide for a more detailed look at what it means.
Test case
The Boardmasters event in Cornwall was a case in point. They screened guests and excluded 465 people with positive LFT’s out of an attendance of 50,000. This equated to the background prevalence in Cornwall at that time, so in that sense, the testing seemed to have done well.
In addition to this they asked for proof of vaccination and the NHS pass. Yet they still had 5000 resultant cases, about 1 in 10 attendees. Attendees were of course, a pretty young and healthy bunch, and at that time largely unvaccinated. It is simply too much to expect to reduce the risk of events like this below what was observed here, apart from, of course, vaccination.

Fair to say that physical distancing was not the top of the agenda….
Yet, the local media reported no increase in admissions, so much natural immunity will have been achieved. I have heard that staff on Plymouth’s ITU noted an increase in admissions in relatives of festival goers, but that is hearsay. Secondary cases were noted far and wide, for example in Swansea. Friends too have had what are called breakthrough infections after vaccination following gatherings. The virus loves a huddle!
Of course, getting together indoors in crowded environments with close contact with hundreds or even thousands of others is testing the process to its limit. Yet life has to go on and the balance in some ways is being established. This is hybrid immunity in action, in other words, accepting spread of infections in the young and lower risk groups and accepting the consequences in terms of viral spread.
What to do
Since the relaxation of restrictions, we are taking risks which are dependent on our ages, vulnerabilities and our day to day contact with loved ones. It is incredibly sensible to get vaccinated, both to reduce the chance of having a nasty infection, the risks of needing hospital treatment, suffering and dying, and the risks to your long term health.
It is also a kindness to those around you as once vaccinated, you are less likely to infect others.
For those who have recovered from infection, then you are likely to have good and enduring immunity, that is if you survived and have not suffered any complications.
For those diminishing number of folk who have not been vaccinated or infected, then testing is sensible. It will tell you when you have an infection and thus help you not infect others, and if negative will give all about as much reassurance as they can.
With testing free right now, there will be many who feel testing before taking any risk is worthwhile and testing is now becoming widely accepted as the norm, in schools, the workplace and elsewhere. For those in contact with elderly relatives, carers and many others is continues to make sense to test freely, despite the wider issues with mass testing.
Of course the other big factor is the level of infection in the areas in which you live, work and play. Right now there is about 1-2% of us with the infection, though many of them will be detected by testing rather than symptoms and this varies from place to place. As prevalence falls the risk drops and vice versa.
Also, as the prevalence of the infection falls, random tests become less useful, and at some point the Government advice may change, particularly with Sunak looking at Boris’s flamboyant and extensive cheque book stubs.

Can I have a quick word Boris!!
So that is the new world of living with endemic COVID.
Optimistically, there are theoretical arguments why this might be as bad as it gets. The virus may – just may – be as virulent as it can get and increasing immunity will reduce it to the rank of a minor infection.
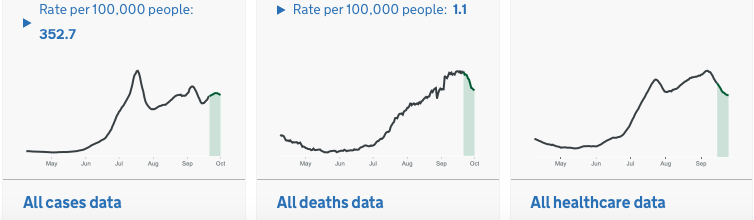
So, although it is not over yet, perhaps this will be the last big wave, and we can deal with new variants as we build up our immunity. Winter will be a test for this. This is how its looking right now:
Boosters are the next issue as the winter comes near, for some they are certainly needed, for others the jury is out.
So fingers crossed for an end to it all, then we can get back to trying to adapt to the monster threats facing all life on this planet. Fuel and food shortages, along with increasing grinding poverty, offer the gentlest of hints at the unadapted future life. That will be the new world of climate change, and that will not nearly be so straightforward.
Endnote…
If you have got to the end of this post, then well done! Feel free to leave any comment or question you wish and I will respond as soon as I can.
In the meantime, I wish you the best of health!