SUMMARY
- Antiviral treatments continue to disappoint.
- Monoclonals have more promise, but are expensive and tricky to give.
- Interesting treatments are emerging, but remain at best, in the pipeline.
- Ivermectin sadly continues to fail when subjected to quality trials.
- Vitamin D remains a safe bet for almost everyone.
- There are treatments in use to manage inflammation and complications.
- Prevention remains better than cure and vaccination is doing that job well.
Introduction
Treating COVID19 has been a tough ask. After all, treatments for any viral infection are few and far between. We can successfully treat HIV, but the those treatments took decades to develop. Acyclovir, for example, is a reasonable treatment for herpes like infections, but otherwise effective anti viral treatments remain elusive.
It is therefore no surprise to me that eighteen months after the arrival of COVD19, direct treatments continue to disappoint. Despite many claims of miracle cures, there remains no simple safe and cheap antiviral to make a real difference to the global pandemic. Some doctors and organisations have taken the stance that anything is better than nothing, particularly in the US where medical over-treatment is pretty much the norm, but the hydroxychloroquine fiasco serves as an example of how this can do more harm than good.

Looking for a cure…..
This post rounds up what treatments are available and the latest trial evidence.
Anti-viral drugs
We didn’t get off to a great start with anti virals. The ineffective antiviral Tamiflu was stockpiled in anticipation of the 2009 Swine Flu epidemic being more transmissible and ended up as a lesson that cost the UK £450m without any real evidence of benefit to anyone – other than the manufacturers bottom line. Interest in SARS antivirals gained funding in 2003, but as that epidemic faded so, shortsightedly, did the funding. The West failed also to respond to the next big warning, MERS in 2012.
Perhaps if either of these infections were more common in the west, funding would have been found, but it wasn’t and research into infections seen as foreign slipped down the priority list.
Then along came COVID19 and some new arrivals. Remdesivir was one of the first great hopes, and is still widely used in the US, despite it being proved not to be good enough for routine use. The WHO Solidarity trial showed it made no difference to mortality, but Tamiflu like, its use continues. Once the full data held by Gilead is released, it may well be seen as another expensive scandalous flop.

Then of course there was the Trump driven hydroxychloroquine saga…….
When it was eventually, definitively and expensively shown to be of little use indeed potentially harmful, its role as a silver bullet was replaced by Ivermectin. The evidence supporting Ivermectin came from small low quality trials and when trials have been better conducted, it has consistently come up short. (See below) It has become emblematic for those who see vaccination as a conspiracy – the mythical simple, cheap, effective and side effect free hero medicine against those nasty corporate vaccines have become one tool by which the pandemic has become politicised, particularly in bipartisan USA.
A new antiviral has been claimed to reduce nasal carriage of the virus, but how this will translate into reducing disease is not yet known and further trials are planned. More promising candidates are in the pipeline, but so far the magic bullet remains evasive.
Manufactured antibodies – Monoclonals
The idea of manufacturing the antibodies we need to neutralise the virus is appealing, but has been fraught with problems and disappointments. Finally in the UK, we have licensed Regeneron, for some reason called Ronapreve over here.
Ronapreve is a combination of two antibodies which stick themselves onto the spike protein and prevent it binding to cells.
Perhaps this has been encouraged by this study which showed reductions in hospitalisation and death of about 70% in high risk patients.It is of course, not, as claimed by the BBC, actually new at all – it was one of the cocktail of drugs used to treat Trump. We have lagged way behind the US and EU in adopting it. Perhaps it will be given in the out patient setting to those at risk and who have not generated any antibodies of their own.
So if you have diabetes, are overweight, have lung disease, or are immunocompromised, this might be something to consider if you develop symptomatic COVID19. It would be worth a call to 111 as soon as your symptoms develop and you test positive if you in those at risk groups.
The cost will always be an issue, but if these reductions play out in the real world, then the £750 (ish) cost of the drug, not counting the cost of administering the one hour infusion, will be well worth it in human and financial terms.
Fluvoxamine
A talk from one of the Together trial leaders reported here, though yet to be published, shows significant promise of a drug called Fluvoxamine, an antidepressant with anti inflammatory actions. Give 739 people testing positive for COVID19 fluvoxamine and 733 a placebo – 77 of the fluvoxamine-takers end up in the hospital; compared to 109 of the placebo group. Not the effectiveness you would expect from an antibiotic, but potentially worthwhile. It is some way from becoming standard use and Im sure more trials will follow.
Metformin
Another more promising drug is Metformin, a widely used anti diabetic medication which has been called a ‘super drug’ due to its widespread benefits in certain situations. In this trial, it showed huge benefit for COVID patients already taking metformin for diabetes. Its use was associated with a reduced mortality by 70% raising the issue that this could also be effective in those with pre diabetes and possible those overweight who are at increased risk of severe infection. This is really promising, particularly as weight (and therefore diabetes etc) has increased during the pandemic.
For people without diabetes, however, results from the Together trial showed no benefit.
Ivermectin
One of the positive outcomes from the pandemic (and there are not that many) is the evolution of well funded platforms to look at repurposing old drugs as well as the new. One is the Recovery Platform, whose largely negative results you can see here. .

The WHO didn’t include Ivermectin its initial study which went on to show the lack of benefit of remdesivir, hydroxychloroquine, lopinavir, and interferon beta-1a.
Pity really as that could have defined its usefulness, or its lack, earlier
The Principle platform have show how the inhaled steroid budesonide can reduce symptoms and are currently investigating Ivermectin. The TOGETHER platform has also been looking at Ivermectin and have found disappointing results. I have posted on Ivermectin before as it has caused controversy all over the world due to some pretty wild claims, varying results, politicised interpretations and a hefty dose of misinformation.
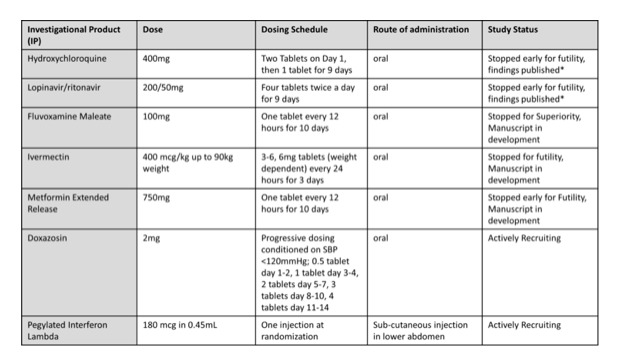
Unfortunately, their evidence shows it doesn’t preventing worsening infection, one of the main claims of its advocates. Of 677 people with Covid symptoms who got high doses for three days, 86 ended up in needing hospital care; in the 678 of the people who got a placebo, 95 did. That’s not a significant difference, and the Together team have duly dropped it from the study. So once again, a well conducted study has shown no benefit. The PRINCIPLE platform will be reporting on its ivermectin trial before too long. However a theme of well conducted trials showing little if any benefit is growing.

Despite this, prescriptions in the privatised US medical system continue to grow, now with exponential growth, mainly in the southern US states.
Ivermectin is attractive to those who have been scared off the vaccine by an effective and well resourced American anti vaccine movement. Prescriptions are increasing and with some getting the stuff from veterinary outlets, (shades of India there) 1,143 Ivermectin exposure cases have been reported to the US Poisons centre due to worries about side effects.
One situation where it might be really useful is for those people with an infestation a roundworm called Strongyloides, particularly when steroids are used. This is far more common in the developing world with poor sanitation and water supply problems where use of steroids can also be dangerously blunderbuss. Treatment with Ivermectin in that situation is can prevent spread of the the worm to cause disseminated infection.

Ivermectin may help anyone in the developing world infected with these worms called Strongyloides stercoralis who go on to get COVID19.
I’m beginning to get the feeling the whole Ivermectin saga will be one of the big pandemic stories once the dust settles. I will write a post on the whole fascinating scenario after the conclusive studies. I suspect it will be along the lines of “Iverdemic- what went wrong and what it means”.
Vitamin D
I continue to be an advocate of Vitamin d as it makes sense on so many levels which drugs like ivermectin do not.
A recent SIGN review has formed the backbone of official advice here, but only really considers bone health, the final sign of vitamin d deficiency. For instance, in wondering wether it reduced respiratory infections at all, they mention: “It is not known if reported effects apply equally to populations from black, Asian and minority ethnic groups or people living with overweight or obesity since data were not available for these population”.

This is despite these populations being at the most risk. Im not suggesting a conspiracy, but they only refer to gold standard RCTs, the availability of which are limited by the vitamins common purchase and use, as well as being cheap. This means the funding for high quality RCTs is difficult to attract.
This is something I first came across after my own diagnosis of MS, in which the potential of Vitamin D to help was clear, but not absolutely defined by definitive trials. For me this showed the limitations of RCT’s, which are crucial when considering widespread use of drugs, but need funding.
So I continue to take vitamin d 5000iu daily as it makes sense for MS and for anyone who spends much time indoors. Remember our light skin is designed for the outdoor life, pretty much from dawn to dusk. Hands up those who live that lifestyle?
Treatments in use
Dexamethase has been shown conclusively to reduce death by 30% when used properly. In well controlled settings this has no doubt been the case. Its global benefit has been reduced by its overuse in less controlled settings and has led to problems with a dangerous invasive fungal illness called mucromycosis in India This is unregulated private medicine at its worst. In effect, making money out of prescriptions that worsen the illness when used outside of hospitals, and causing side effects needing expensive and often unaffordable hospital treatment.
Colchicine, a cheap anti gout drug, was considered too, but also failed to impress in trials.
Americans, always the first to medicines, for better and for worse, have generated much hot air on treatment in an effort to deny medical impotence. The “you’ve got do do something Doc!” phenomenon. At the forefront is guidance from a group called FLCCC, which includes, in addition to Ivermectin, steroids and anticoagulants which are widely used without the need for high publicity, poorly evaluated protocols. They also recommend Vitamin C and zinc, though there is not much evidence of their benefit in hospital treatment.
I described the rationale behind the use of vitamin C at home early in the pandemic, zinc too, but as ever, the people whose nutrition is so poor that they would benefit most, will also be the ones least likely to supplement. The Inverse Care Law in action.
Prevention
An ounce of prevention is worth a pound of cure, said Benjamin Franklin centuries ago and remains as true as ever. Of course, keeping as healthy as you can is as important as ever too, but this in not straightforward for many living in what I certainly consider to be a sick society. With climate change racing in unchecked, it may even be terminally ill, but thats another matter.

Vitamin D deficiency, so common in our world is certainly a marker for ill health, but can be surprisingly low in people who are otherwise healthy. Unlike Ivermectin, there is a sound scientific basis for getting enough Vitamin D either from sun or supplements. Unless, that is you are lucky, or foolish enough to have enough of the worlds declining oily fish in your diet.
It continues to make sense to supplement, including in children. This will ensure the immune benefits of vitamin D are ready to go if you happen to get infected, or indeed vaccinated. As we enter the endemic phase, it will be one or the other, and possible both.
Vaccination
This is the best tool we have to prevent infection, it has reduced spread, and dramatically reduced hospital admissions and death. With the delta wave crashing across the US, the difference between states less or more heavily vaccinated is surfacing and certainly adds to the case against widespread American anti vaccine sentiment.
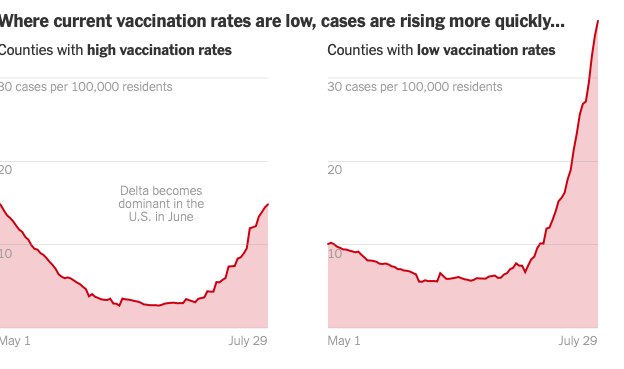
In the USA, it seems states where less people are vaccinated are having many more COVID19 cases. Look here for more details.

and the difference is also seen in deaths with far less deaths in the more vaccinated states.
So vaccination is continuing to offer a safer route to immunity than natural infection which though less with the Delta Variant, still appears to be good at keeping people out of hospital and cutting mortality. It is also likely to reduce transmission, though with less effectiveness than before.
There are also emerging studies, here and here showing that long term immunity after vaccination is likely due to the persistence of memory cells which will be able to produce antibody producing cells and killer cells which will protect vaccines when they come across the virus. That is good news.
Conclusion.
Direct treatments for SarsCov2 have been disappointing and few have made a significant impact. Despite all the hope and some incredible hype, therapies still mainly focus on treating inflammation and complications of the illness. An effective antiviral would be fantastic for those with the illness, though costs are likely to be high. So for now it’s as important as ever to keep yourself as healthy as you can. Vaccination and Vitamin D continues to make sense.
Finally…..
If you have got this far, thanks for reading the post. If you have any comments or questions, feel free to use the box below and I’ll get back to you as soon as I can
I wish you the very best of health.