Summary
- The new deal we have with the virus is now playing out.
- No restrictions, reduced mask wearing and mass gatherings mean the fifth wave is different from the others.
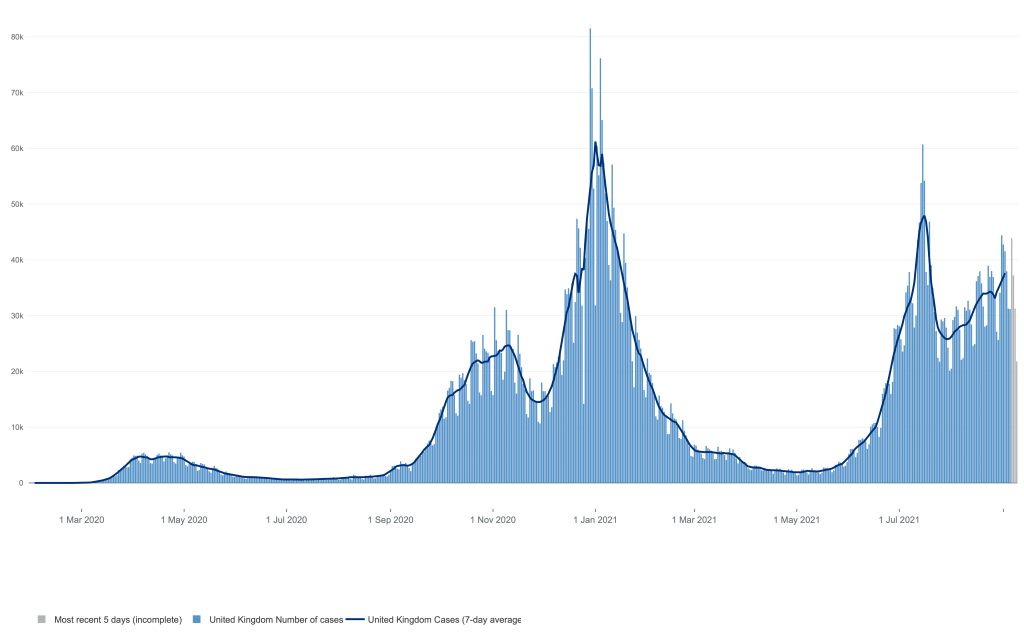
- It is clear from this that vaccinations are working well and that lockdowns in the past had a significant effect.
- Reinfections after vaccination or infection are less severe – this means the disease is becoming milder.
- The NHS pass is far from perfect but will be coming soon.
- The NHS is under threat like never before and is set for further privatisation.
Introduction
My last post included a note of optimism that the fifth wave might have peaked, but sadly the downward trend was a two day blip. What we are seeing is the number of cases, admissions and deaths slowly creeping up which is different to the rapid increase and decline we have seen in the past. The new deal with the virus has changed things – we have a long slow wave whose duration is difficult to predict.
30,000 daily positive tests, not all of whom will have symptoms. With school testing now, we can expect more asymptomatic cases which may not translate into hospital activity.

Far less admissions – 1000 yesterday – than before, though COVID cases still occupy 7% of hospital beds.

And, largely thanks to vaccination, far fewer deaths – now running at about 150 a day.
The word Endemic is derived from the greek for ‘native’ and means that the virus is here to stay with infections occurring at a regular rate, rather than the more explosive epidemic, or global pandemic.
With the kids now back at school and universities ready to accept admissions, there are plenty of reasons to assume this will carry on for some time. We are doing a new deal with SARS2. The question is how will the health sector, and its exhausted staff cope with a steady 7% or so of hospital beds occupied with COVID patients and what are the implications for us all…..
Is how things are when a virus becomes endemic?
What this means
Being endemic, it means that anyone who has not had the infection or been vaccinated will eventually come across the virus and become infected.
There is evidence that we are on the way with this, over 90% of blood samples taken randomly from adults containing anti covid antibodies – this is good news. Yet, 10% of people represent 6.4 million people with no protection, and some of these antibody levels may be declining with time. Some too have not been generated by infection with the Delta variant – so this phase of the pandemic will be a balance between many competing factors.

There will be a balance between viruses and antiviral antibodies.
That we will all be infected or vaccinated also is important when balancing the risk of vaccination versus infection. For people with MS, for example, there is a definite but small risk of relapses after vaccination, which is a worry, though this is far less than the risk of similar problems after the infection, so the vaccination continues to make sense even with reports of problems making the news.
I sometimes wonder, hope indeed, that Delta might be the variant most adapted to us in terms of infectivity – in other words is it possible that Delta represents ‘peak infectiveness’? This opinion paints an optimistic picture, that this might be as infective as SARS2 can get. Hope rains eternal!
The problem of course, is that the NHS is creaking already. GP’s are retiring early, worn out by the ever increasing workload, even pre-covid. They are not being replace in sufficient numbers to cover losses, and there are shortfalls in the hospital sector also. Recruitment is difficult and posts are empty. The endemic phase will be draining for a demoralised staff, in particular as we have only just entered Autumn.
Epidemic of the unvaccinated?
PHE data from August shows that there were 113,000 cases in the vaccinated, and 219,000 in the unvaccinated. This translated into 3172 and 5064 admissions respectively. In other words, 61% of hospital admissions between February and August were in the unvaccinated. In terms of the pandemic this is encouraging as more people are still getting vaccinated. Given the unvaccinated population is far smaller, and far younger right now, this shows the benefit of vaccination once again.

Vaccination is the main contributor to reduced admissions and deaths
Most deaths are in the vaccinated – once again, the vaccinated population are more numerous, older and more vulnerable so this is to be expected. Just 3% of deaths in the vaccinated were under 50, as opposed to 18% in the unvaccinated. Trial and real world evidence shows that most of these the deaths are preventable by vaccination and so many of these personal tragedies could have been avoided with a relatively simple intervention.
Re-infections happen after wild (natural) infection, but are not so bad.
Public Health England Data from July shows that the rate of reinfections in those who have already had COVID19 have increase from 0.6% with the Alpha variant to 1.2% with the dominant Delta strain. By that they mean people who have had positive tests more than 90 days apart – on this basis there have possible been 23,000 reinfections, though not all are certain as they have not all been genomically tested. Data from ONS also suggests that reinfections are milder, at least in term so having less viral load.

In other words, immunity after wild infection is good but not perfect. Given that about 18% of the immunity out there comes from wild infection, this is good to know.
PHE suggest the chance of spreading your infection to a household member is only slightly more with Delta with the ‘secondary attack’ rate increased from 10 to 11% . This will of course, be dependent on the number of people in the house, crowding, vaccination status and general health.
Breakthrough infection after vaccination are not so bad either
Breakthrough infections are occurring due to expected levels of vaccine failure, the new variant, and possible some waning of immunity from the vaccine. Thankfully they seem to be less severe, according to the Zoe symptoms tracker who report:

“fewer symptoms were reported over a shorter period of time by those who had already had a jab, suggesting that they were falling less seriously ill and getting better more quickly.“
This is to be expected, having any immunity is better than none and though breakthrough infections are increasing, they gladly seem not so severe. Vaccines are doing a very good job at preventing serious illness.
Schools in
It continues to be the case that kids do welll with COVID infection, thanks in part to their ready to go defences being far more potent than adults. Despite this ,3,550 children have been admitted to American hospitals, 2% of the total.
As further disruptions to education should be the number one priority to avoid. It may also be reasonable for children to achieve immunity from natural infection which will benefit them as the years go by. It seems to me that this is happening. Despite the widespread testing before the Boardmasters festival, there followed thousands of cases, and its reasonable to assume that the virus will spread amongst schoolchildren until most if not all have been infected.

Hands up those who haven’t read the JCVI statement on vaccinating 12-15 year olds.
This will be impossible to prevent in primary schools, and very difficult in secondary schools. In universities, it will be mitigated by increasing levels of vaccination. In all cases, infection will lead to immunity and in terms of the hybrid policy of vaccination and infection now playing out, it seems to be that widespread testing in school, with half hearted isolation is somewhat quixotic.
More so indeed, after the JCVI, the independent experts on vaccination, ruled that the benefits of vaccination in the 12-15 year bracket are marginal at best.
Passports out
So now we are entering the realm of passports, that demon of those who see conspiracy. These are being taken up throughout out the world and will shortly be introduced in the UK, with nightclubs and crowded indoor venues being asked to insist on them. So what are the conditions needed for the NHS pass?
Put simply:
- 2 doses of the Moderna, AstraZeneca or Pfizer vaccine
- one dose of the Janssen vaccine
- proof of natural immunity shown by a positive PCR test result for COVID-19, lasting for 180 days after the date of the positive test and following completion of the self-isolation period
This needn’t be as divisive as it seems. We all need passports to travel, and all sorts of ID to do all sorts of things. We have masses of data on spending and travel recorded on our mobile phones, and our computerised world is developing incredibly rapidly with each of us generating thousands of data points as we go about our business. The NHS pass is another example of how technology is marching on, destination uncertain.

Coming to a mobile near you?
The NHS pass would be improved by increasing the 180 days to any positive PCR test in the last year, or perhaps longer. Including the possibility of a recent negative test to allow entry to venues would mean that no-one, other than those acively infected and without immunity would be barred and be acceptable to all other than those who believe it is all a backhand method of surveillance.
Undoubtedly the passport includes an element of coercion for younger people to get vaccinated, but evidence shows that a history of wild infection should enable freedom from any restrictions too. Further, as vaccinated people can transmit the virus (albeit less likely to) none of this is absolute.
For indoor venues, the bedrock of our cultural life, this will be a way of avoiding financial ruin at at time when further restrictions, whatever Boris Johnson might say, are on the table as the winter approaches.
There is no way to have zero risk, but the passports seek to reduce it to a manageable level. So far, I have not needed mine, delaying my application till I do and though it’s a tough time for the arts, as many will still avoid crowded venues.
Levelling down rant
Just as the pandemic has taught us that inequality and poverty leads to more spread, more cases and more deaths, the government is unlearning the lessons and intentionally increasing both.
Not extending the £20 increase needed to cover increased costs due the pandemic will hit the very poorest people in society. Not content with that, the NI increases said to fund the social care crisis will also be levied from working people with lower earners paying proportionally more that the better off.

Sadly, primary care in this country is in crisis too. I bumped into a former bright and empathic colleague about to retire with the sad feeling of leaving a sinking ship, much as I felt when I retired a few years ago.
Your local GP, the bedrock of first contact when unwell or struggling, is increasingly unlikely to be someone you know. Cynically, though not without good reason, I see the run down of primary care, indeed the whole stressed out NHS as preparation for further privatisation.
I find it hard to imagine how primary care will work without doctors getting to know their patients and vice-versa. No amount of information technology will replace that human familiarity which seems to be fading fast.
Patients ‘levelled down’ will be finding it more difficult to seek out the services they need to cope, survive even. It’s as if nothing has happened over the last eighteen months. Some dogma is built to last.
It seems so long since a Labour government, many youngsters will not have experienced anything than endless, destructive, free market conservative leadership which this pandemic has aptly demonstrated, is getting us nowhere.

The enormous challenges of the future requires new thinking, yet policy seems forever to hark back to the pristine self serving socially isolated, molly coddled playing fields of Eton.
Feedback
Thanks for reading this post. If you gave any comments questions or feedback, do drop me a line in the box below and I’ll get back to you as soon as I can. Stay as well as you can!
BREAKING NEWS
One thing you can rely on the government is chaos. Despite all the statements about passports going ahead, it seems Sajid Javid has now stated, on todays Andrew Marr show, that they will not be. Perhaps that is a good thing as it seems to me they have been badly thought out, perhaps because the realities of night club life are a long way from those Etonian playing fields…..or maybe its this????
For this multiple sclerosis-focused installment, we interviewed Claire S. Riley, M.D., medical director of the Columbia Multiple Sclerosis Center in New York, NY. Here’s what she had to say:
HealthCentral: Could the COVID vaccine cause a flare-up or make my MS symptoms worse?
Claire S. Riley, M.D.: Just to level set, we don’t have much information about how the COVID vaccines currently approved in this country potentially impact individuals with multiple sclerosis. People with autoimmune disease were largely excluded from all the global clinical vaccination trials, so we operate in a data-free zone here.
From:
https://www.healthcentral.com/article/covid-vaccine-with-multiple-sclerosis
Thanks for this. They state “We are in alignment with the National MS Society’s recommendation for MS patients to get vaccinated, and we think that the risk that patients will have an attack of MS related to the vaccine is relatively low.”
Of course there are risks with the vaccine, but there are far bigger risks with COVID19, particularly with anyone with disabilities or other illnesses. Anyone on DMT’s needs to seek advice on which vaccine and when as ability to produce antibodies will vary.
“There were PROBABLY no more than 4 or 5 people with MS in the trials”
This isn’t science this is guessing!
“The Pfizer trials were of about 40,000 people, and assuming a prevalence of MS of 1:1000, then they would have included 4-5 people with MS. Just a guess but likely to be about right.”
Thanks Mr Truth, indeed it guessing, thats why I said it’s a guess and I must say with an incidence of 1:1000, there would be 40 (not 4!) people randomly chosen in that sample, you are right, they are usually excluded from trials as the trials look at safety and effectiveness in the general population. In any case, small numbers would not be enough to make any conclusions. The evidence anyone with MS needs has come from real world data and is well described in the MS Blog (https://multiple-sclerosis-research.org/?category=covid-19&s=). I thoroughly recommend a visit there if you have MS and are interested to find out more. Vaccination remains far less risky than wild infection. I hope this helps.
Wow, I can’t get over the vast amount of information here in your blog. Im one of the 140,000+ people in the UK with Multiple Sclerosis. Im keeping away from vaccines because some of the ingredients are awful (formaldehyde in the flu vaccine was one of them – this was the reason I stopped getting the flu jab a few years ago). I also cannot not find any data on how many MS’ers were in the vaccine trials. My neuro/doctors are also at a loss with this one. Im not saying never, just being very, very cautious and collecting as much info as I can. – Your blog is amazing by the way.
Thanks for your kind words. The best source of COVID/vaccine information for people , like us with MS is the MS blog written by team at Bart’s. (link below) There were probably no more than 4 or 5 people with MS in the trials, too small to draw any conclusions, but my understanding is that we should do as well as anyone else unless we have other problems or are on certain therapies.
https://multiple-sclerosis-research.org
Thanks again
Thank you. Can I ask – re. the 4/5 people on the trials – where were you able to get hold of this info? Was this also through Barts? My other question and no-one seems to be able to answer this is – I am not taking any DMTs. My neuro thinks I probably have SPMS. How do I find out what vaccine others in my situation have gone for? and how they got on with it?
Hi Fran, The Pfizer trials were of about 40,000 people, and assuming a prevalence of MS of 1:1000, then they would have included 4-5 people with MS. Just a guess but likely to be about right. Far too few to be analysed. I get the feeling that is would be very hard to find out what others with MS have gone for. My friends with MS (10-20) have all been vaccinated, none with any problems that I have heard of, but that’s anecdote. Have you looked at lifestyle and MS – OMS is probably the best organisation which focuses on this? Vitamin D too is certainly worth taking for anyone with MS.
Hi Fran,
Here is an article written about the vaccine & M.S. that may be helpful:
https://www.healthcentral.com/article/covid-vaccine-with-multiple-sclerosis
Here is an excerpt from it answering the question of how many people with M.S. were in the trials:
For this multiple sclerosis-focused installment, we interviewed Claire S. Riley, M.D., medical director of the Columbia Multiple Sclerosis Center in New York, NY. Here’s what she had to say:
HealthCentral: Could the COVID vaccine cause a flare-up or make my MS symptoms worse?
Claire S. Riley, M.D.: Just to level set, we don’t have much information about how the COVID vaccines currently approved in this country potentially impact individuals with multiple sclerosis. People with autoimmune disease were largely excluded from all the global clinical vaccination trials, so we operate in a data-free zone here.