SUMMARY.
- The fourth wave looks very different from the last three with younger populations testing positive.
- This matters for schools, currently in chaos due to testing policy.
- Certification of infection or vaccination looks increasingly likely.
- COVID19 has an impact on the brain.
- More mischievous pseudo-science regarding ‘vaccine related deaths’ debunked.
- Vaccination does reduce transmission.
- Treatments and trials. Ivermectin and others in the pipeline
- Vaccines for children – a good thing – I’m not convinced?
- Aerosol spread and why masks work.
- Our wonderful immune system.
Fourth wave rolls on. Or does it?
Well the fourth wave rumbles on with prediction that it might peak at 70,000 cases a day by the end of July. The shape of the curve seems pretty much as before, apart from two important things. One is that hospitalisations and deaths, while increased, remain at a low rate and are only increasing slowly. The other is the interesting ‘heat map’ of just who the positive cases are. The diagram looks a bit unwieldy, but basically the darker the colour, the higher the number of cases, the higher up the older the case, and time from left to right.
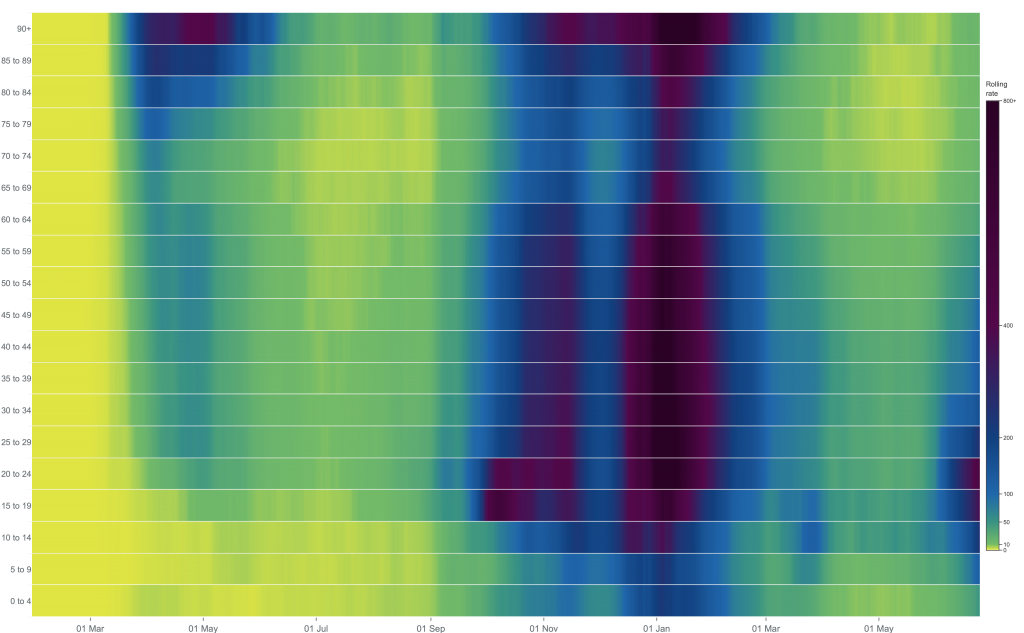
It is a nice representation of the end of the first wave, with mainly the elderly being tested, then the second and third waves starting in September and late December respectively. The fourth wave, on the far right is different. Most of the positive results now being from 10-24 age group. In other words, students and school kids.
That goes some way to explain why the cases do not end up in hospital or worse and not something I hear much on the news. It also highlights the good news that older and more vulnerable age groups are relatively well protected, either by having had the infection before (at least 4 million people) or been fully vaccinated, now almost 33 million people. The down side of course it the huge number of viruses present in each case, all of which increases the risk of variants and the problems they bring, worries persist with the Delta variant, but so far so good.
Schools in….
Given all that, it not only seems reasonable to allow further release of restrictions as planned, but it will also be politically expedient for the new Health Secretary to beat an optimistic drum and distract from the fall of the Matt Hancock whose familiarly in the public eye magnifies the misuse of public cash for his own ends. (literally, it seems)

The deployment of the much criticised lateral flow tests so beloved by the disgraced Hancock seems to be messing up education. Far too many children are off school, 5% right now, about 350,000 kids in total. This can reasonably be seen as a adverse effect of a terrible testing policy. Twice weekly testing has led to bubbles, often including 200 or so children going home to isolate for a week after a single positive test.
Youngsters in big, crowded institutions tend to spread viral infections and COVID is no exception. Vulnerable children and all adult staff should now be protected with vaccination and spread in schools seems inevitable, as shown above. There is some evidence too that children suffer long covid as much as adults, with this study suggesting more than half can still have symptoms 120 days after infection.
The politicians have suggested daily testing for all kids and isolation only of those positive, but the tests will miss many cases so I wonder how useful this will be. Almost as an aside, the US FDA has banned the use of our Innova tests which they suggest should now be binned due to serious errors in the manufacturers claims.
Passports out…..
The issue of covid passports has come into the public eye once again as an understandably Delta phobic EU is introducing restrictions of those seeking to travel to Europe from the UK. I should mention that this environmentally destructive addiction is partly at least due to the very high cost of UK holidays. A week in a Cornish caravan can cost over £1000, a sum far higher than the average package holiday to Costa Del Somewhere. Plus of course, ugly living and working environments leaves many desperate to get away. the need for vaccine passports, or evidence of previous infection, will raise howls from libertarian’s whose continue to campaign for the freedom to do anything anywhere any time. Much of this was for so many an illusion, but a vaccine certificate is generally well supported along with our low levels of vaccine hesitancy.
COVID19 and the brain
For anyone who thinks that COVID19 is just a flu like illness this study should give pause for thought. They looked at people in the UK Biobank who had brain scans before the pandemic, and rescanned those who went on to get COVID19. They found significant changes in the grey matter in defined areas of the brain. While the changes are significant, the overall impact on those individuals may not be so worrying. Other infections can case similar changes also and these can return to normal with time, which may be why brain fog eventually clears. A brain healthy lifestyle remains as important as ever.
Mischief….
A widely quoted study showing that for every three covid deaths we have two vaccine deaths is utter nonsense and once again shows how some pretty terrible opinion can masquerade as science. We can all come to whatever opinions we like, but my misinformation posts are driven by stuff like this which is plain wrong. How can it even get published? There are now a plethora of publishing platforms that publish and peer review articles; let’s say some are more selective than others. This paper resulted in two members (now increased to six) of the vetting board quitting in disgust after realising platform’s peer review was flimsy enough to let this sort of scare story stuff through. The whole notion is expertly and interestingly debunked here and includes the following tweets:

Transmission benefits of vaccination
I always thought that vaccination would lead to less transmission of infection by reducing viral load, and now this study proves it. If you get vaccinated, you are 40-50% less likely to pass it on to household members. The reduction in transmission is likely to extend to contacts outside the household too, though this was not in the study.
It was large study involving nearly a million contacts of 100,000 cases so the findings are robust and encouraging news for the vaccines. Interestingly, the BioNTec and Oxford vaccines seemed to do the job equally well. The full results are here:
Heart inflammation
Apart from the clotting issues, another rare side effect of vaccines has emerged. In the US there has now been 1200 cases of inflammation of the heart called pericarditis, with most cases being mild and as of June 11th, 9 people were in hospital with the condition and two in intensive care. So, for anyone developing chest pain after the vaccine, particularly the second Pfizer or Moderna vaccine, seek advice early. The risks are more for men under 30, where the risk is 1 in 30,000.
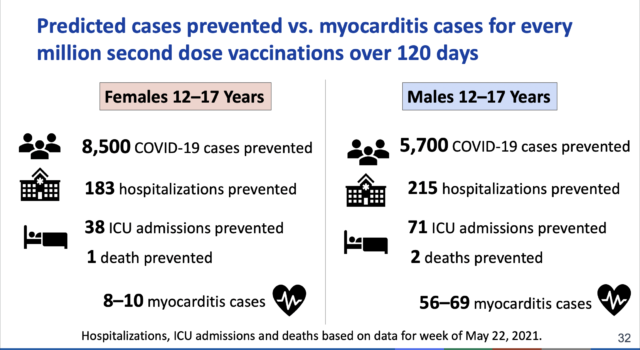
The CDC also note that 2,767 people aged 12 to 29 years old have died from Covid since the pandemic began and this graphic shows the risk-benefit to the young from vaccination. The risk benefit ratio clearly changes the younger you are, but the graphic does not include long covid which can affect more children than we hoped with almost half having chronic symptoms 4 months after a positive test.
There have been three cases of numbness of the face shortly after the Oxford vaccine, representing a Guillain Barre type syndrome seen more frequently after the 1976 Swine flu vaccine and a rare feature of many vaccines. No cause for alarm there, but it is important to report anything you think may be caused by the vaccine to our yellow card system, though with serious side effects, this is usually done by health care staff.
Treatments
The Principle trial platform has defined the best treatment for COVID19 and happily one result shows that simple treatment with a steroid inhaler offers significant benefits, reducing the duration of illness by three days in those treated. Results on hospitalisation are awaited, but is reported to have reduced admission from 10.3 to 8.5%. This is a useful treatment for anyone vulnerable or suffering significnat COVID19 symptoms.
The Recovery team have decided to move on to the controversial Ivermectin (IVM). Hopefully this will define its place in treatment if it has one. A recent review continues to define the drug as the “new Hydroxychloroquine”. Their conclusion is:
“The few existing higher quality clinical trials testing ivermectin against the disease uniformly have failed to find a positive result. It’s only the smaller, lower-quality trials that have been positive. This is a good indication that the drug probably doesn’t work.”
There is another IVM trial going on in Canada with the lead there stating on radio that he suspects it will show benefit, but only enough to recommend more research. Let’s hope the Recovery trial of Ivermectin will be the final chapter in this story, though some pretty terrible reporting of the drug and its trials continue to dominate antivaxx websites, with their usual selective use of trials, dodgy references and hyperbole. I don’t think we will ever see an end to that.
The ongoing use of Remdesivir in the USA, even though no longer recommended by the WHO as a useful treatment describes how once a medication is in use, it is hard to stop due the culture of prescription and the “You’ve Got to do Something Doctor” syndrome. One small uncontrolled Phase 1 study in the US reported resolution of symptoms in 10 patients who were treated with the ‘old’ anti-inflammatory cyclosporin. Another observational study suggests it could be an interesting and cheap option, but like so many small studies, it is interesting, but hardly a basis for widespread treatment. It demonstrates the need for public funding of properly powered trials of which Principle and other platforms are perhaps a start. Repurposing of drugs already available could be a rich vein.
Whatever the trial of Ivermectin finds, I expect that its use will continue as will claims based on dubious trials and anecdote. Unless of course the Recovery trial is positive. I hope it is, but given what has already been published, Im not biting my nails.
Trials…..
It is time to reflect on how successful the vaccine trial were. Perhaps we have learnt how to shrink the sometimes hopelessly long timescales previously needed for clinical trials and extend the compressed scheduling, again along with public investment and an effective research infrastructure to antibiotics and other therapeutics. That would be a positive spin off from the pandemic. Indeed, this was on the table at the recent G7 meeting in Cornwall. The UK government supports the Global Antibiotic research and Development partnership a multi-sector body whose aims include developing treatments for antibiotic resistant infections and getting those antibiotics to those who need them. £1million donated by the UK is hardly a fortune, but its a start.
Vaccines for children
We are now offering vaccines to all adults and there seem long queues around the country suggesting uptake, in the UK at least, will be good. I’m sure much of this is a drive to get back to normal rather than a precise understanding of biology, but does show a high level of trust in the vaccine. The next consideration is whether to vaccinate children.
There are three issues for me. One is does the vaccine do children more harm than good. Clearly the balance will be different from adults as children seems to deal with the infection well. There are exceptions with the MIC syndrome tragically affecting some children. A CDC study back in August 2020 of 576 children hospitalised with SARS-CoV-2 infection reported a lower hospitalisation rate compared with adults (8 versus 165 per 100 000); however, one in three hospitalised children required admission to intensive care units, a rate similar to adults.
It may even be desirable for children to build up immunity through infection as this will serve them well into the future when new variants may come along. There is also the vexed issue of whether to vaccinate children who have already had infection – it might be a good idea to test them first.

So the next question is whether immunising children will help the whole of society? In other words, do children transmit the infection? In secondary and primary schools they seem not to.
Perhaps schools are different from super-spreading events, the same kids go to the same school every day. I remember well the flood of infections opened at the start of school term, so Im sure that they do spread viral illnesses, but mainly amongst their peers and they deal with it well.
The third issue is whether or not they area priority group? It’s a global pandemic and in global terms they are certainly are not anywhere near as high up the list as the billions of unvaccinated vulnerable and their health care workers around the world, including plenty of vulnerable young people, so the answer is no.
Further, a review in the BMJ stated the potential advantages of infection in early life:
“Once most adults are vaccinated, circulation of SARS-CoV-2 may in fact be desirable, as it is likely to lead to primary infection early in life when disease is mild, followed by booster re-exposures throughout adulthood as transmission blocking immunity wanes but disease blocking immunity remains high. This would keep reinfections mild and immunity up to date.”
There are exceptions of course. There are vulnerable children who have been isolating for far too long while waiting for a vaccine. Those with lung disease and other vulnerabilities may well benefit from vaccination. Vulnerable parents and carers would, in the vast majority of cases, be vaccinated already.
Aerosols and masks
It appears that SarsCov2 is spread by small aerosols rather than the larger droplets which spreads flu. This means they are more likely to be emitted while talking and breathing if infected and travel that little bit further. This adds to the evidence that wearing masks makes sense, though something better than cloth masks are needed for health care workers.
A recent study showed that fabric face masks “blocked between 62.6% and 87.1% of fine particles, whereas surgical masks protected against an average of 78.2% of fine particles. N95 masks blocked 99.6% of fine particles” and added to more evidence that masks make a significant difference.

Perhaps FFP type mask (right) for healthcare staff and those at risk and surgical masks (left) for others.
Wearing them indoors in crowded places makes sense, and the higher the number of ongoing infections, the more sense it makes. The results from mass gatherings seems mixed, with Scottish visitors to the recent England vs Scotland game causing an uptick in infections, while the FA cup final only saw a handful of cases, though conclusion from this are shaky as the testing system failed.
Good news.
An interesting paper here describes how immunity after infection can be long lived. Although the median age of the 77 participants was 46 and they had not been severely affected by their COVID19, the prolonged cell based immunity they describe is good news. Perhaps not too much of a surprise as most people do well with the infection and we know reinfection is not common, though new variants can change that. One of the problems is that immune response varies considerable after infection, but is much more predictable after vaccination. Also, not vaccinating those who are antibody positive could speed up vaccine roll out in nations who are struggling.
Antibody levels in the blood are not everything. Further evidence that T cells are key players comes from looking at the response to infection of people on treatment which essentially reduce B cell populations, for instance in MS. It seems that those on immunotherapy with a less potent B cell response, compensate with a more robust T cell response. Im constantly amazed by our wonderful immune system.
Our other systems of course, are equally intricate and all work like clockwork to keep us alive and well, at least until they fail due to bad luck, genes or commonly because of unhealthy lifestyles and our essentially unhealthy society. Work from the Zoe team show how diet really make a difference with higher levels of vegetable and fruit intake important, more so for those at the poorer end of society hit hard by the pandemic.
Once again, it’s going to be an interesting month……
Thanks for an upbeat message, one based on reality, not on hyperbole and deception as we have so often been subjected to.
Here is an other study showing the virtues of a p3 mask
https://www.authorea.com/users/421653/articles/527590-ffp3-respirators-protect-healthcare-workers-against-infection-with-sars-cov-2?commit=e567e67501cd6ee0dd1a6e8e4acdf2c4fd70e0ec
Thanks Owen. Thanks for the reference – glad the masks are effective. I agree there is a lot of hyperbole around!
Thanks once again for a very comprehensive overview