Summary
- The damaging effects of the British empire remain relevant to our relationship with India.
- India is in the news due to record COVID19 caseloads and inadequate health sector.
- Our links with India made any Indian variant more likely to emerge in the UK and once again we have been very slow to restrict travel.
- The new B1616.2 variant may increase cases, but the vaccine is likely to be at least partially effective against it. (Fingers crossed!)
We have history –
History emerges in its written form, some time after the event. For me, reading “Inglorious Empire” by Shashi Tharoor was an eye opener, describing in vivid detail why the British Empire was designed in every aspect of its function and structure to suck the life blood out of its colonies. Our exploitation of India over three centuries financed much of our own Industrial development the empires expansion. Prior to the arrival of the East India Company in 1612, India, though in a weakened condition with the Mughal empire in crisis, was still the biggest exporter of goods in the world and arguably the most advanced civilisation. In 1700, India accounted for 27% of the world economy. Their vast industry and exotic produce drew the British to ever more intrusion, violence, domination and ultimately conquest and looting on a grand scale.

Just one of Queen Victorias birthday presents – Memorials such as this dedication to Queen Victoria were paid for by looting of the Indian economy, its resources and its people.
For a comprehensive description of the disaster, read Tharoor’s, “Inglorious Raj”
By the time the British were removed, an astonishing 335 years later, India was on its knees. Indeed, Tharoor feels is yet to fully recover. He argues that poverty and inequality have persisted due to post-colonial structures which have not been dismantled. However, one metric has certainly improved – deaths due to famines were a regular feature of life in India under he Raj, but they have not happened since independence. Partition and war, both legacies of British rule, have had their dreadful toll, but the pandemic is exposing structural weaknesses in India that recently has been drawn to nationalism and boasting.
With the establishment of the Commonwealth, an alliance of over 50 former colonies, whose wealth, in spite of the misleading name, did and continues to flow to the west. Until the Commonwealth Act of 1962 and 1968, immigration to the UK was understandably extensive and so we have become a multicultural society with 1.2 million Britons of Indian ancestry with continued links to their families remaining at home. With India’s economy expanding, Boris is keen to meet Modi and expand trade, albeit perhaps now more on Indian terms than in the past. That was, until the pandemic arrived.
Indias pandemic
The first wave of Indias pandemic was met with a sudden and complete lockdown which stranded many itinerant workers and caused much suffering in a crowded and disjointed nation. However, it helped manage the first wave and give Modi a premature opportunity for triumphalism which seems a common feature of many right leaning politicians. India has a younger population than the West and so the number of deaths per head of population is going to be inevitably lower with a disease that affects the elderly. Even so, their pandemic has rapidly overwhelmed the health sector. With the second wave, Modi’s early boasts have now with turned to humiliation and structural weaknesses, like our own, have been brutally exposed.
Although their rate of cases and deaths are far lower than ours, (first graph), the huge numbers involved is mind boggling (Second graph). They recorded the highest daily number of cases anywhere in the world in April 26th – 360,960 people and after 22 million infections, have recorded over 260,000 deaths already. Right now the number of cases is 326,000 with 3780 deaths. It is widely acknowledged that these numbers will be an underestimate. Running out of beds and oxygen in many hospitals has left patients totally vulnerable to their fate.
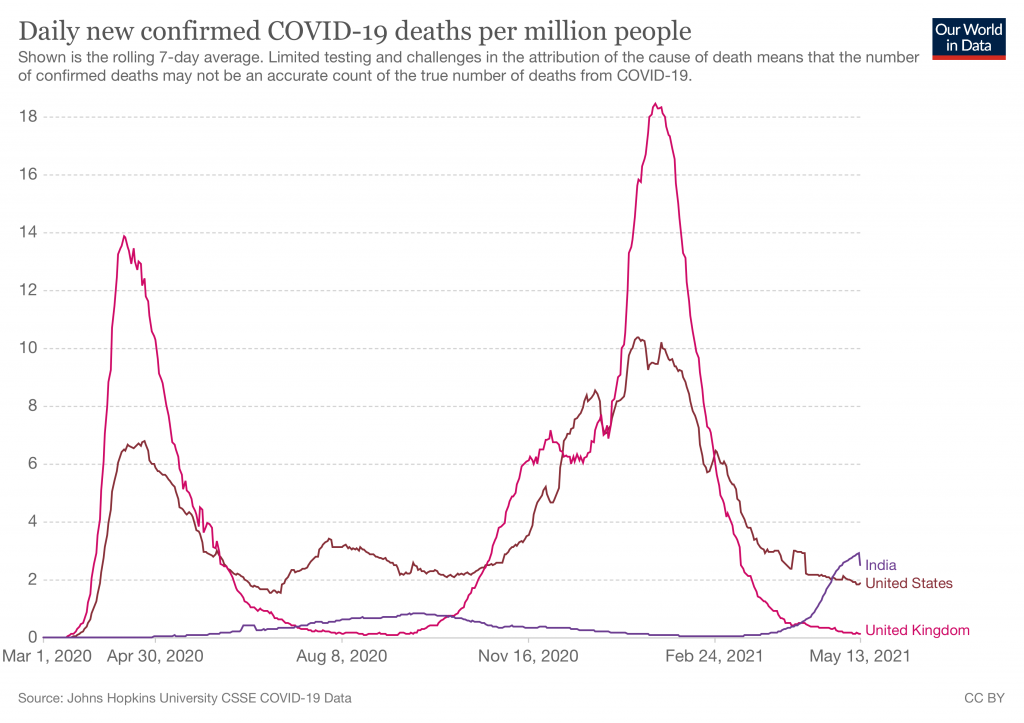
RATES – If India were to have the same per capita mortality as the UK, they would be heading for 2.5 million deaths – but with a younger population this is unlikely.

NUMBERS – The second wave in India, in terms of numbers of people suffering, is potentially devastating. This does not take into account significant undercounting. Ignore the downtick, a sudden drop like this is likely to be an artefact, or due to a change in counting or perhaps political interference..
So what has happened?
After the first wave, infections were thought to have affected up to 50% of urban dwellers but have now spread to the Indian countryside where there is very poor access to healthcare. As in the UK, but of course on a much bigger scale, the opportunity to establish Testing Tracing and isolation schemes was not established after the first wave and Indian testing is running at very low levels – 1.7 million tests in total up till April 27th, compared to the UK’s 500,000 PCR tests a day. They are clearly not testing enough people (over 20% of their tests are positive), while we are testing too many. Small fires were not extinguished and now they have an outbreak raging out of control.
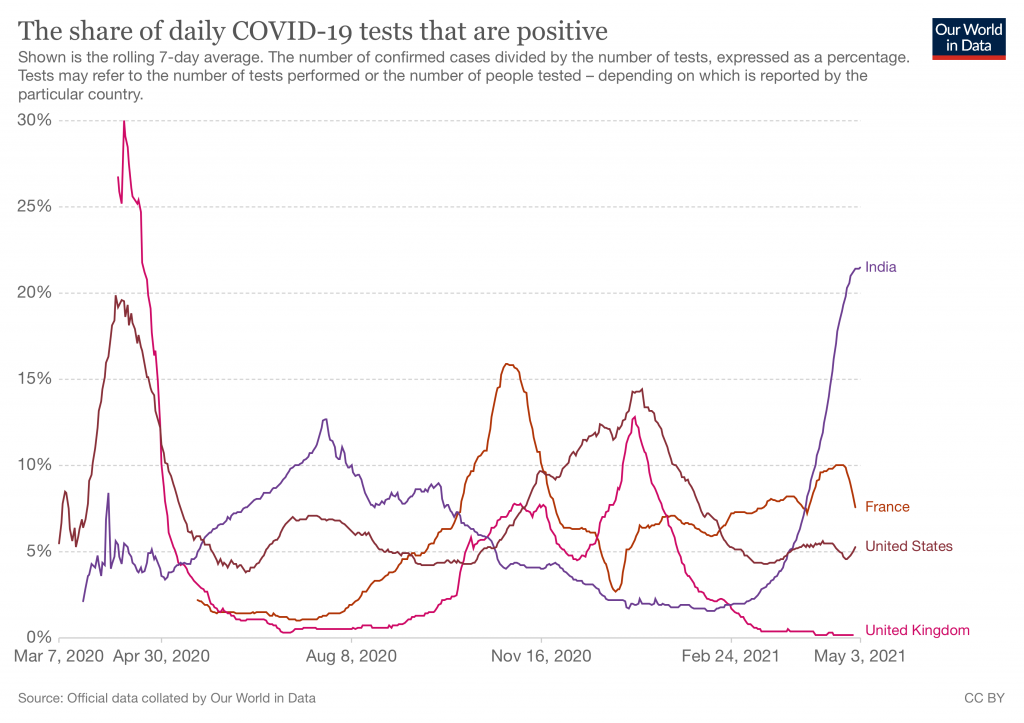
TESTING – About 1 in 5 tests in India are positive due to less screening, and testing on demand for those who are symptomatic – many cases are not detected or traced and so the virus spreads.
Warning bells should have rung as the Indian health sector is a shadow of that in the West – they spend just 1% of the GNP on healthcare as opposed to our 9.5%. They also have injustice built into their system with private hospitals for the wealthy and insured and public hospitals for those who are not. Hence the hideous sights of overwhelmed hospitals. It takes little imagination to appreciate the horror of losing someone who might have been saved with simple respiratory support, or gasping your last while waiting in vain for help. India is said to need 500,000 ICU beds to cope with people needing complex respiratory support – they have just 90,000, all of which are now occupied. They have only 40,000 ventilators available for 1.3 billion people. (One per 30,000 people as compared to our one per 7000)The potential for an expanding calamity looms large and the counting of cases and deaths is know to be considerably underestimated.
Like almost everywhere, Vitamin D levels in the Indian population are low. There is of course, far more sunlight in India than the UK, yet the indoor lifestyle is common, urban pollution, poor diet and too much skin covering are other factors in reducing immune boosting exposure to sunlight. Like here, the issue, a significant marker for risk, is marginalised despite its potential to make a significant difference.
Bad medicine is common. Patients are prescribed many useless drugs, including hydroxychloroquine, 7-8 drugs including ivermectin, doxycycline, azithromycin, and favipiravir, making treatment for mild illness paradoxically expensive. The rich are over-treated, and the poor under-treated if treatment is available. The culture encourages pointless intervention and polypharmacy. The notion that the small first wave was thanks to these interventions has now been debunked.
A terrible example of the consequences of bad medicine in the emergence of a previously rare fungal infection called mucormycosis due to the toxic cocktail of people weakened by COVID19, combined with the rampant overuse of antibiotics and steroids. It is a terrible infection, treatable with an anti-fungal which is in short supply and very expensive to manage as surgery is needed to remove infected tissue.
Impressive local production of Remdesivir, and Tociluzumab are overwhelmed by the sheer volume of hoarding and inappropriate use. Useless drugs add to the patients medical bills and useful treatment is not given at the right time. Stable paying patients are admitted needlessly while other die for the lack of simple interventions like oxygen.
Indias new variant
Add to the contribution caused by the spread of the UK “Kent” variant to India, there is a new Indian variant named B1617.2; it is termed a double mutant as it has two significant amino acid changes on its spike. This emphasises the poiint that the more people you have with active infections, the more change there is to generate mutations, some os which will spread more quickly and become dominant. This, together with the UK variant, seem more contagious and worryingly there are concerns that this wave is affecting younger people. There have also been reports of reinfections suggesting potential evasion of naturally acquired immunity.

COVID’S SPIKE – This is what the spike looks like as it sits on top of the viral membrane. The green bits are glucose like molecules which provide camouflage. It is the exposed purple bits that vaccines and treatments can target.
A study in March 2021 found reinfections affected 4.5% of 1,300 health workers, many of who had no symptoms first time around suggesting some evasion of immunity gained from the first infection in some cases. With few restrictions in travel and a wide diaspora, the UK, South African and Brazilian strains are circulating in India, but added to this is their own B1617.2 strain which is becoming dominant in many areas. With testing and sequencing at very low levels, it is hard to be sure, but the second Indian wave seems to be pointing to a more dominant strain. It does seem to spread rapidly, it is already evident in 40 other countries and already being transmitted within the community in the UK. However the UK government might claim their measures were adequate, they have not prevented the spread of the variant into the UK and once again, slow decision making will have costs.
Oxygen
Oxygen is a vital treatment for at least 41% of people admitted to hospital with COVID19, and the supply problems of oxygen in India has highlighted the neglect in in its provision. Rather than invest in Oxygen concentrating plants to supply oxygen in bulk, many hospitals rely on cylinders which are 5 times more expensive, and vulnerable to surges in demand. This has been costing lives throughout the developing world for decades and has now been highlighted by the pandemic. Eight months into the pandemic, 33 of the planned 160 oxygen concentration plants have been commissioned have been installed and I suspect that deaths due to lack of this most basic of treatments will continue.
Vaccination
India has set a target of vaccination 250 million people by July, and 117 million have received their first dose. They have been slow to import the vaccines which would have been useful earlier, even if only for the urbanites who would could afford them, as this would have spared at least some of the healthcare capacity so needed now. They have now stopped exporting vaccines and the government have belatedly given a £400m grant to the Serum Institute of India to increase production. Perhaps they believed their own rhetoric about having beaten the pandemic earlier and so saw their impressive vaccine industry as a big earner rather than a healthcare need.
They are also importing Sputnik vaccines to increase supply, but even if they could suddenly invent all the vaccines they need, there are not enough vaccinators to deliver them, so progress is likely to be slow. A first come first served approach to vaccination ensures those who need them most are shunted back in the queue. The central government has bought vaccines for those over 45 and those at risk, but the rest are left to local governments with vastly differing finances and health infrastructure to buy for themselves.

Covaxin, a vaccine developed and manufactured in India with an efficiency of 81% estimated from interim results of their phase 3 trials, may come to the rescue. It’s rather like the Sinovac, an inactivated viral vaccine with low production costs. It costs £2.90 per dose compared to £20 for Moderna and £26 for the Pfizer. Bharat biotech reckon they can make an impressive 300million doses by the end of the year.
Perhaps there are signs they might be some slowing down in the rate of increase, but counting is unreliable and many COVID19 deaths will go unrecorded. Overall about 20% of deaths are certified with a medical cause and this drops to 5% in more remote regions. There are many reasons for this and government figures don’t tally with local data.
To add to the human impact are reported shortages of wood traditionally used to cremate the dead. The consequent shortage of trees means damage to habitats and we are back to the start of the pandemic caused by pressure on the natural world and in particular bat populations. Of course, we in the UK have little to shout about here with our very low levels of tree coverage, but I wonder how long it will take for this out-dated culture to change or will religion trump science, as it so often does.
So what now?
It may be that the second wave in India is beginning to peak. It is hard to be certain, but cases and deaths continue. If the wave now declines that will be good news, and perhaps, like the first wave, its natural history might not be fully understood, but vaccinating the vulnerable and health care workers will have made a significant difference.
As for now, we in the UK will have to wait and see if the new variant does manage to evade vaccines or previous immunity. With T cells induced by vaccines active against most variants so far, it looks to me like the new variant will lead to more infections in the unvaccinated, uninfected and unlucky, but for those protected by natural infection or vaccination, it may not be such a problem. I hope I’m not wrong! This is important as for most nations there is a long way to go before herd immunity, which is a flexible concept at best, and ultimately depends of those you are in contact with. It will vary locally and with time, so it seems to be fading from view as a useful pandemic defining concept.

Back to the history I mentioned at the beginning of this post. 83 years ago Ghandi visited Bolton and spoke to British workers who might have been aggrieved at his attempts to undermine British exports of cotton to India. They understood that he was right to ensure Indian weavers produce linen out of Indian cotton. 83 years later the link between India and Bolton again comes to light with the B1617 outbreak threatening to halt or slow down the end of lockdown there.
Prior to the pandemic 2,500 people people would fly to India daily and this was reduced only by about half after our Kent variant driven surge over the new year. This incredible level of travel delivered the Kent variant to India, and recent belated restrictions have led to the B1617.2 virus spreading here.
The consequences of unregulated global commerce, slow decision making and global travel continue to unfold.
I started this post with the thought that it takes a long tome for real history to be written. Perhaps soon the place of the British empire and other empires in creating an unequal, diminished world will be more widely recognised. B.1617.2, our most recent import from India reminds me that this is a global pandemic, that we are a global species, and that we are still a long way from properly addressing our past, as well adapting to our future.